

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Among clavicle fractures, 69% occur in the diaphysis, 28% in the distal and 3% in the proximal position.1) Segmental fractures involving the distal and the proximal ends of the clavicle are even rarer. The injury mechanism is often unclear and the management of these fractures remains controversial. We report two cases with a segmental fracture are described: One patient was treated conservatively and another patient was treated operatively and both of all, excellent results were achieved. The management of segmental clavicle injuries is discussed.
Case Reports
1. Case 1
A 40-year-old man presented to the outpatient clinic with pain over the right clavicle following a history of fall from height. There was no external wound. Physical examination revealed tenderness on proximal and distal portion of the clavicle. Movements of the shoulder joint were restricted due to referred pain in the clavicle. There was no evidence of neurovascular deficit and no other significant combined injuries.
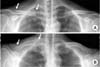
Radiographs showed a segmental fracture clavicle with lateral and medial end of clavicle (Fig. 1). Computed tomography showed segmental proximal and distal fracture with displacement, especially proximal end (Fig. 2).
Initially, we planned operative treatment for the fracture. But he refused operative treatment under anesthesia. So, we changed the initial plan. Within 2 weeks after trauma, if the degree of displacement is more progress than initial radiography, we plan to perform operative treatment. He was applied figure-eight-bandage to prevent shortening of clavicle for 8 weeks. We checked the radiography of the clavicle weekly. Fortunately, the degree of displacement was not more progress than initial radiography. He removed the brace at the time of 8 weeks after trauma. After 3 months later, he was able to move full range of motion. At the last follow-up (3 years after trauma), we checked the radiography (Fig. 3).
2. Case 2
A 62-year-old male, right hand dominant, presented to the emergency department with pain over the right clavicle following a history of bicycle accident. There was no external wound. The skin was not at risk.
Physical examination revealed tenderness on right mid shaft and distal portion of the clavicle. Movements of the shoulder joint were restricted due to pain. There was no evidence of neurovascular deficit and no other significant combined injuries.
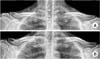
Radiographs showed a segmental clavicle fracture with distal end and mid-shaft of clavicle (Fig. 4). Computed tomography showed mid-shaft and distal fracture with displacement, especially distal end (Fig. 5).
We planned operative treatment for the fracture. Operation was performed under general anesthesia in a beach chair position. Closed reduction and percutaneous pinning with a Steinmann pin of mid-clavicle fracture was done. Open reduction with pinning and wiring of distal clavicle was done. Post-operative radiograph showed the final fixation achieved (Fig. 6).
Postoperatively, the arm was supported in an arm-sling, with the patient instructed to perform regular hand grasping and elbow range of motion exercises, as well as gentle pendulum exercises of the shoulder. After then, passive stretching exercise and strengthening exercise were followed. The patient had pain-free full range of movement of shoulder joint after 12 weeks.
Discussion
Clavicle fractures are common, comprising 2.6% of all adult fractures. Midshaft clavicular fractures are the most common, ranging from 69% and 82%, distal fractures comprise 21% to 28%, and proximal fractures occur between 2% and 3%.1) The segmental clavicle fracture is an uncommon pattern. One study reported that 0.8% of clavicle fractures was segmental.2)
Clavicle fractures are usually caused by a direct trauma to the shoulder, but the mechanism of injury leading to a segmental clavicle fracture is not well understood. Some reports described that this type fracture occur due to two separate concurrent forces.3) One is direct force on the point of the shoulder girdle due to fall. The other is an indirect force, which may give rise to clavicle fractures by the shearing force delivered from the humerus to the sternum.
Fractures of the proximal clavicle are difficult to visualize because overlying structures in the chest obscure the view of the proximal end. For rare proximal fractures, particularly those that extend into the sternoclavicular joint, a Hobb's view or a serendipity view or computed tomography scan may be helpful to access the fractures and identify their relationship to the sternoclavicular joint. Recently, one reported a case of neglected segmental clavicle fracture.4) According to the report, initially operation was performed on distal end of clavicle using hook plate. After operation, patient had ongoing pain over the medial clavicular region. He underwent operative treatment for medial clavicle fracture on 6 weeks later after initial injury. We recommend that physician examine carefully including tenderness on ipsilateral sternoclavicular joint for the patient of clavicle fracture. This simple step is very helpful for management of clavicular fracture and avoidance of misdiagnosis.
The management of segmental fractures has little standard guidance in the literature, with some reports of successful operative35) and non-operative management.6) Miller et al.5) presented a report of fracture of the medial and lateral extremity of the clavicle with the use of a reconstruction plate and another with locking T-plate. Authors emphasized that due to the rarity of the case, there is no routine surgical technique described for the treatment of this type of fracture. Recently reported cases were summarized (Table 1).4678910) According to previous reports, operative treatment overweighted than conservative treatment. Operative technique was plate and screw on proximal lesion in all cases and K-wire fixation on or hook plate on distal lesion.
In this report, we compared two possible methods, one operatively and one conservatively treatment, for the rare fracture pattern of clavicle. And the results showed excellent outcomes for both treatments. The treatment should be based on the individual fracture pattern and patient characteristics.





 XML Download
XML Download