

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
This study was to evaluate the radiological and clinical mid-term results and the presence of post-traumatic osteoarthritis after osteosynthesis in patients under the age of 50 years undergoing osteosynthesis for distal femur intra-articular fractures (AO/OTA 33-B & C) from high-energy trauma.
Materials and Methods
Between January 2008 and January 2013, a total of twenty-one patients with more than three years of follow-up were enrolled. Recovery of the alignment of the lower extremity, union period, and the presence of post-traumatic osteoarthritis were confirmed by follow-up radiographs. Clinically, the range of motion, pain on fracture lesion, and Knee Society score (KSS) were evaluated.
Results
The average duration of union was 18.2 weeks (10-28 weeks), and the alignment of the lower extremity was within normal range in all patients. Seven patients showed post-traumatic osteoarthritis at the final follow-up after more than three years. The presence of post-traumatic osteoarthritis was associated with the classification of fractures, coronal plane fracture, and age. The average range of motion, knee score among KSS, and function score at the last follow-up were 128.7°, 86.1, and 85.1, all showing a greater improvement when compared with the one-year follow-up scores.
Figures and Tables
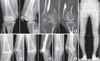 | Fig. 1A 46-year-old female with metaphyseal simple and complete articular fracture with coronal plane fracture, who was injured by a fall (AO/OTA 33-C3). (A) Anteroposterior and lateral radiograph of the right distal femur fracture. (B) Computed tomography. (C) Radiographs, obtained immediately operatively, show an internal fixation. (D) Radiographs obtained at 10 months after surgery show complete bony union at the fracture site. (E) Radiographs obtained at 14 months after surgery show a device removal status. (F) Radiographs obtained at 4 years after surgery show normal alignment and no post-traumatic osteoarthritis progression.
|
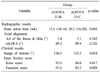
Table 1
Radiographic and Clinical Results between the AO/OTA 33-B and C Groups
![]()
Table 2
Selected Variables in Accordance with the Result of the Stepwise Method of Multiple Logistic Regression (Dependent Variable=Post-Traumatic Osteoarthritis Change)

![]()
Table 3
Comparison of Pain at the Fracture Site Pain between Short Term and Mid-Term
![]()
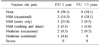
Table 4
Comparison of the Knee Society Score between Short-Term Result and Mid-Termz

![]()
References
1. Martinet O, Cordey J, Harder Y, Maier A, Bühler M, Barraud GE. The epidemiology of fractures of the distal femur. Injury. 2000; 31:Suppl 3. C62–C63.

2. Stover M. Distal femoral fractures: current treatment, results and problems. Injury. 2001; 32:Suppl 3. SC3–SC13.
3. Vallier HA, Hennessey TA, Sontich JK, Patterson BM. Failure of LCP condylar plate fixation in the distal part of the femur. A report of six cases. J Bone Joint Surg Am. 2006; 88:846–853.
4. Krettek C, Schandelmaier P, Miclau T, Bertram R, Holmes W, Tscherne H. Transarticular joint reconstruction and indirect plate osteosynthesis for complex distal supracondylar femoral fractures. Injury. 1997; 28:Suppl 1. A31–A41.
5. Anderson DD, Chubinskaya S, Guilak F, et al. Posttraumatic osteoarthritis: improved understanding and opportunities for early intervention. J Orthop Res. 2011; 29:802–809.
6. Rademakers MV, Kerkhoffs GM, Sierevelt IN, Raaymakers EL, Marti RK. Intra-articular fractures of the distal femur: a long-term follow-up study of surgically treated patients. J Orthop Trauma. 2004; 18:213–219.
7. Kim JJ, Choi JH. Treatment of distal femur fracture. J Korean Fract Soc. 2011; 24:288–293.
8. Nork SE, Segina DN, Aflatoon K, et al. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. J Bone Joint Surg Am. 2005; 87:564–569.
9. Shon OJ, Kwon MS, Park CH. Comparison of results of minimally invasive plate osteosynthesis according to types of locking plate in distal femoral fractures. J Korean Fract Soc. 2012; 25:269–276.
10. Afsari A, Liporace F, Lindvall E, Infante A Jr, Sagi HC, Haidukewych GJ. Clamp-assisted reduction of high subtrochanteric fractures of the femur. J Bone Joint Surg Am. 2009; 91:1913–1918.
11. Cherian JJ, Kapadia BH, Banerjee S, Jauregui JJ, Issa K, Mont MA. Mechanical, anatomical, and kinematic axis in TKA: concepts and practical applications. Curr Rev Musculoskelet Med. 2014; 7:89–95.
12. Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. (248):1989; 13–14.
13. Gwathmey FW Jr, Jones-Quaidoo SM, Kahler D, Hurwitz S, Cui Q. Distal femoral fractures: current concepts. J Am Acad Orthop Surg. 2010; 18:597–607.
14. Guy P, Krettek C, Mannss J, Whittall KP, Schandelmaier P, Tscherne H. CT-based analysis of the geometry of the distal femur. Injury. 1998; 29:Suppl 3. C16–C21.
15. Kolb K, Grützner P, Koller H, Windisch C, Marx F, Kolb W. The condylar plate for treatment of distal femoral fractures: a long-term follow-up study. Injury. 2009; 40:440–448.
16. Pettine KA. Supracondylar fractures of the femur: long-term follow-up of closed versus nonrigid internal fixation. Contemp Orthop. 1990; 21:253–261.
17. Siliski JM, Mahring M, Hofer HP. Supracondylar-intercondylar fractures of the femur. Treatment by internal fixation. J Bone Joint Surg Am. 1989; 71:95–104.
18. Starr AJ, Jones AL, Reinert CM. The "swashbuckler": a modified anterior approach for fractures of the distal femur. J Orthop Trauma. 1999; 13:138–140.
 XML Download
XML Download