

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Generally, lateral plating is used for a comminuted fracture of the distal femur. However, in some cases, it has been shown that using a medial plate is necessary to achieve better outcome. Nevertheless, there are no available anatomical plates that fit either the distal medial femoral condyle or fracture fixation, except for the relatively short plate developed for distal femoral osteotomy. We found that locking compression plate-proximal lateral tibia (LCP-PLT) fits anatomically well for the contour of the ipsilateral medial femoral condyle. Moreover, LCP-PLT has less risk of breaking the thread holes since it rarely needs to be bent. We report a plastic bone model study and two cases of distal femoral fractures fixed with medial plating using LCP-PLT.
Figures and Tables
Fig. 1
Photographs of the femur bone model (3B Scientific, Hamburg, Germany) with various plates on medial condyle, locking compression plate-proximal lateral tibia (LCP-PLT), tomoFix-medial distal femur plate (TomoFix-MDF), proximal humerus internal locking plate system (PHILOS), LCP-medial distal tibia plate (LCP-MDTP), LCP-distal metaphyseal tibia (LCP-DMT), and LCP-distal tibia T (LCP-T) plate, in order from upper left corner.

Fig. 2
Photographs of the femur bone model (3B Scientific, Hamburg, Germany) showing the application of locking compression plate- proximal lateral tibia (LCP-PLT) on appropriate position. A: Distal posterior hole.

Fig. 3
Photographs of the femur bone model (Synbone, Malans, Switzerland) with the application of locking compression plate-proximal lateral tibia (LCP- PLT) on appropriate position. A: Distal posterior screw directed to the intercondylar notch, B: 2nd row screw reached the lateral femoral condyle without penetration into the intercondylar notch.
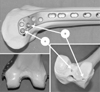
Fig. 4
Radiographs of the right knee and the right femur showing preexisting lateral plate and comminuted fracture of the right distal femur.
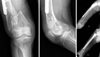
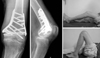
Fig. 5
Radiographs and photographs of the right femur at 12 months after the surgery showing good fracture healing and good range of motion of the right knee.


References
1. Singh AK, Rastogi A, Singh V. Biomechanical comparison of dynamic condylar screw and locking compression plate fixation in unstable distal femoral fractures: an in vitro study. Indian J Orthop. 2013; 47:615–620.

2. Ha SS, Sim JC, Hong KD, Kim JY, Park KH, Choi YH. The surgical treatment of distal femur medial condyle fracture using lateral anatomical plate of opposite side through medial approach. J Korean Fract Soc. 2009; 22:246–251.
3. Boulton CL, Kim H, Shah SB, et al. Do locking screws work in plates bent at holes? J Orthop Trauma. 2014; 28:189–194.
4. Checroun AJ, Mekhail AO, Ebraheim NA, Jackson WT, Yeasting RA. Extensile medial approach to the femur. J Orthop Trauma. 1996; 10:481–486.
5. Schatzker J, Lambert DC. Supracondylar fractures of the femur. Clin Orthop Relat Res. 1979; 138:77–83.
6. Yune SH, Rhee KJ, Park CH, Byun KY, Lee SY, Rho SK. Importance of maintenance medial buttress in treatment of supra-condylar and inter-condylar (T-condylar) fracture of the femur. J Korean Soc Fract. 1996; 9:50–58.
7. Visser J, Brinkman JM, Bleys RL, Castelein RM, van Heerwaarden RJ. The safety and feasibility of a less invasive distal femur closing wedge osteotomy technique: a cadaveric dissection study of the medial aspect of the distal femur. Knee Surg Sports Traumatol Arthrosc. 2013; 21:220–227.
8. Jiamton C, Apivatthakakul T. The safety and feasibility of minimally invasive plate osteosynthesis (MIPO) on the medial side of the femur: a cadaveric injection study. Injury. 2015; 46:2170–2176.
9. Kim JJ, Oh HK, Bae JY, Kim JW. Radiological assessment of the safe zone for medial minimally invasive plate osteosynthesis in the distal femur with computed tomography angiography. Injury. 2014; 45:1964–1969.
 XML Download
XML Download