

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A pseudoaneurysm of popliteal artery may originate from a perforation caused by traumatic injury around knee joint or iatrogenic after total knee arthroplasty,12) insertion of intra-medullary nail,34) or reconstruction of anterior cruciate ligament.5) However, a pseudoaneurysm after conservative management of distal femur has been rarely reported. We describe herein a case of a huge popliteal artery pseudoaneurysm that occurred eleven months after the conservative treatment of a distal femur fracture.
Case Reports
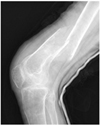
A 60-year-old female presented with left knee pain in outpatient clinic. Two months earlier she sustained slip-down injury from wheelchair; however, she did not visit hospital because she regarded the injury as a simple contusion. Furthermore, she had been unable to walk for ten years due to bilateral lower extremity paralysis caused by tuberculous spondylitis. Continuous knee swelling and pain prompted her to ask a medical advice two months after initial trauma. On the plain X-ray, distal femur fracture with severe displacement was observed (Fig. 1).
Beside bilateral lower extremity paralysis, she also had tuberculosis-destroyed kidney resulted in chronic renal failure relying on hemodialysis. She had the history of chronic tuberculosis and secondary bacterial infection around urinary tract and psoas muscle area additionally. Due to her chronic medical conditions including chronic renal failure on hemodialysis and latent and recurrent tuberculosis infection and to low functional demand of lower extremity from bilateral paralysis, conservative treatment with cast after closed reduction was initiated. Immobilization with long leg cast was maintained for 6 weeks. Her periodic follow-up was lost for a while. After eleven months from the trauma, the patient visited again the outpatient clinic with complaint of a tender swelling over the posterior side of left distal thigh; Plain X-ray revealed an ovoid soft tissue shadow (3 cm) behind the fracture site under an impression of residual hematoma. The fracture site had little callus with impression of non-union on plain X-ray (Fig. 2).
On physical examination, she had a large pulsatile mass on the medial aspect of the left distal thigh (Fig. 3A). A computed tomography (CT) scan revealed a huge mass-like lesion communicating with the popliteal artery in the left popliteal area, implying a pseudoaneurysm originated from the popliteal artery adjacent to the site of the fracture of the femur (Fig. 3B, C). The diameter of pseudoaneurysm was approximately 15 cm.
The patient was referred to vascular surgeon and underwent surgical exploration, aneurysmectomy, and popliteal angioplasty. Internal fixation of fracture site could be not performed due to inadequate bone stock for rigid fixation and high morbidity expected after bone surgery. An incision was made along the marked line through the course of the popliteal artery over the pseudoaneurysm to block the femoral arterial forward and backward flow. After clamping the femoral artery and popliteal artery, the pseudoaneurysm was resected and was deemed to originate at the site of a defect on the arterial wall of popliteal artery (Fig. 4A). Finally, angioplasty was performed directly by an oblique resection of the defect margin (Fig. 4B). Anticoagulation therapy with aspirin and clopidogrel (Plavix; Handok, Seoul, Korea) was initiated after the surgery. At 3-month follow-up, CT angiography revealed the good patency of popliteal artery. Although, fracture non-union is maintained, there was no discomfort in keeping pre-injury activity. Until recent follow-up (2-year after operation), there was no gross evidence of recurrence of pseudoaneurysm.
Discussion
Superficial femoral artery or popliteal artery pseudoaneurysms are generally considered to be the sequelae of arterial injury caused by a laceration of the arterial wall and the formation of a hematoma in the adjacent tissues. The popliteal artery or femoral artery is vulnerable to accidental injury during surgical procedure around knee joint and femur. Several case reports in the literature have described how pseudoaneurysm around femur occurred after surgical management on the knee and femur. Inter-locking screw during the insertion of femoral intra-medullary nailing was reported as one of cause of small size artery pseudoaneurysm.467) Various locations were reported from proximal portion to distal portion through length of femur regarding to the location of interlocking screw. Usually the small sized vessel is injured during insertion of inter-locking screw. During total knee arthroplasty or high tibial osteotomy, popliteal artery or the geniculate artery could be also damaged.28)
However, the development of spontaneous pseudoaneurysm without surgical procedure is rarely reported. In our case, the pseudoaneurysm of popliteal artery might have occurred by sharp edges of fracture during initial injury or later displacement of fracture fragments. We initially treated this fracture with conservative measure due to her medical conditions. Because she did neither bear weight nor walk, the deformity after mal-union or prolonged time to union was not considered problematic. However, the sharp beak of unstable fracture site seemed to cause the repetitive injury of arterial wall. Therefore, when we counsel the medically poor condition patients with conservative option, the possibility of major vessel injury by unstable fracture fragment in situation of delayed or non-union should be kept in mind. Surgical stabilization would be the better choice in this case when we retrospectively criticize the adequacy of the treatment procedure. Nevertheless, we did not provide the rigid fixation in second chance during aneurysmectomy due to her medical condition and poor bone stock again.
Compartment syndrome of posterior compartment was also reported.9) Although the size of pseudoaneurysm in our cause was very large, due to paraplegia, the compartment syndrome was not meaningful for this patient and the vascular insufficiency of lower extremity was not observed.
The detection time of traumatic pseudoaneurysm varies from hours to years, depending on the regions involved and the clinical symptoms and signs that are manifested, including enlarged pulsatile swelling, palpable thrill, pain, edema, and compressive neuropathy. In the present case, the patient had been in a wheelchair for 10 years due to tuberculous spondylitis and the time took longer to detect the pseudoaneurysm than that usually experienced in other trauma patients. The rarity of this complication, as well as the time interval required to induce the pseudoaneurysm might explain the frequent delayed diagnosis.
The treatment of pseudoaneurysm depends mostly on their location and size. Small asymptomatic lesions may simply be observed constantly for 4 to 6 weeks until spontaneous recovery occurs; however, interventions are generally indicated for larger (>3 cm) symptomatic lesions or those in which vital vasculature is involved. Current therapeutic methods include ultrasound-guided compression, ultrasound-guided injection of thrombin, endovascular repair using coil embolization or insertion of a stent-graft, or open surgical repair.2810) In the present case, open surgical aneurysmectomy and angioplasty were performed because of the large size of the pseudoaneurysm (>10 cm) and its late detection.
In conclusion, we present the case of a rare post-traumatic pseudoaneurysm of the popliteal artery that was successfully managed through open vascular surgery. Although some traumatic vascular lesions are often detected tardily because of their insidious onset and variable clinical presentation, as seen in our case, progressive pulsatile swelling around the fracture site should raise clinical suspicion and lead to a prompt investigation.



 XML Download
XML Download