

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Regardless of the efforts of several treatments after pelvic bone fracture, as many as 5% of all pelvic fractures result in malunion or nonunion of the pelvis. These complications can cause disabling symptoms, including pain, instability, and gait disturbance, which can decrease life quality of patients and increase socioeconomic problems. Therefore concerns regarding the treatment of malunion and nonunion after pelvic bone fracture are increasing. We report our experience and surgical management for pelvic malunion and nonunion.
Figures and Tables
Fig. 1
Correction of malunion and nonunion after pelvic bone fracture can be achieved with a variety of bone clamps and reduction forceps.

Fig. 2
Radiographs show posterior translation of the left hemipelvis on anteroposterior and inlet view and 5.5 cm significant superior migration of the left hemipelvis on outlet view. LLD: limb length discrepancy.

Fig. 3
Two-dimensional computed tomography shows nonunion through the left sacrum and left pubic ramus and 20 degree internal rotation deformity.
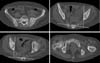
Fig. 4
Three-dimensional computed tomography shows superior and posterior migration along with internal rotation and flexion deformity of the left hemipelvis.



References
1. Min BW, Song KS, Kang CH, Kim YS. Operative treatment of the unstable pelvic bone fracture. J Korean Fract Soc. 1996; 9:518–524.

2. Min BW, Kang CH, Shin HK. Complication of the operative treatment in unstable pelvic bone fractures. J Korean Hip Soc. 2004; 16:373–379.
3. Cole JD, Blum DA, Ansel LJ. Outcome after fixation of unstable posterior pelvic ring injuries. Clin Orthop Relat Res. 1996; (329):160–179.
4. Lindahl J, Hirvensalo E, Böstman O, Santavirta S. Failure of reduction with an external fixator in the management of injuries of the pelvic ring. Long-term evaluation of 110 patients. J Bone Joint Surg Br. 1999; 81:955–962.
5. Matta JM, Dickson KF, Markovich GD. Surgical treatment of pelvic nonunions and malunions. Clin Orthop Relat Res. 1996; (329):199–206.
6. Mears DC. Management of pelvic pseudarthroses and pelvic malunion. Orthopade. 1996; 25:441–448.
7. Pennal GF, Massiah KA. Nonunion and delayed union of fractures of the pelvis. Clin Orthop Relat Res. 1980; (151):124–129.
8. Vanderschot P, Daenens K, Broos P. Surgical treatment of post-traumatic pelvic deformities. Injury. 1998; 29:19–22.
9. Asprinio DE, Helfet DL, Tile M. Complications. In : Tile M, editor. Fractures of the pelvis and acetabulum. 2nd ed. Baltimore: Williams & Wilkins;1995. p. 224–245.
10. Stover MD, Matta JM. Malunion and nonunion of the pelvis: posttraumatic deformity. In : Tile M, Helfet D, Kellam J, editors. Fractures of the pelvis and acetabulum. 3rd ed. Philadelphia: Lippincott Williams & Wilkins;2003. p. 400–408.
11. Gautier E, Rommens PM, Matta JM. Late reconstruction after pelvic ring injuries. Injury. 1996; 27:Suppl 2. B39–B46.
12. Altman GT, Altman DT, Routt ML Jr. Symptomatic hypertrophic pubic ramus nonunion treated with a retrograde medullary screw. J Orthop Trauma. 2000; 14:582–585.
13. Hallel T, Malkin C. Fatigue fracture of the pubic ramus following total hip arthroplasty with unusual delayed healing. Clin Orthop Relat Res. 1982; (166):162–164.
14. Pavlov H, Nelson TL, Warren RF, Torg JS, Burstein AH. Stress fractures of the pubic ramus. A report of twelve cases. J Bone Joint Surg Am. 1982; 64:1020–1025.
15. Mears DC, Velyvis J. Surgical reconstruction of late pelvic post-traumatic nonunion and malalignment. J Bone Joint Surg Br. 2003; 85:21–30.
16. Oransky M, Tortora M. Nonunions and malunions after pelvic fractures: why they occur and what can be done? Injury. 2007; 38:489–496.
17. Mears DC, Velyvis JH. In situ fixation of pelvic nonunions following pathologic and insufficiency fractures. J Bone Joint Surg Am. 2002; 84-A:721–728.
18. Rousseau MA, Laude F, Lazennec JY, Saillant G, Catonné Y. Two-stage surgical procedure for treating pelvic malunions. Int Orthop. 2006; 30:338–341.
19. Vrahas M, Gordon RG, Mears DC, Krieger D, Sclabassi RJ. Intraoperative somatosensory evoked potential monitoring of pelvic and acetabular fractures. J Orthop Trauma. 1992; 6:50–58.
20. Beaulé PE, Antoniades J, Matta JM. Trans-sacral fixation for failed posterior fixation of the pelvic ring. Arch Orthop Trauma Surg. 2006; 126:49–52.
21. Westphal T, Piatek S, Winckler S. Pseudarthrosis of an occult fracture in zone III of the sacrum. Unfallchirurg. 1999; 102:493–496.
22. Kanakaris NK, Angoules AG, Nikolaou VS, Kontakis G, Giannoudis PV. Treatment and outcomes of pelvic malunions and nonunions: a systematic review. Clin Orthop Relat Res. 2009; 467:2112–2124.
23. Tile M, Pennal GF. Pelvic disruption: principles of management. Clin Orthop Relat Res. 1980; (151):56–64.
 XML Download
XML Download