

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Anteromedial force to the knee in an extended position can cause an avulsion fracture of the proximal fibula with combined injuries to the posterolateral ligaments. Avulsion fractures of the proximal fibula are rare and current management of these fractures is based on few descriptions in literature. Various surgical methods of fixation for these fractures have been reported, but there is still no standard treatment modality. Anatomic reduction of these fractures is technically difficult, and failure of reduction may cause posterolateral instability, secondary arthritis and other complications. We present our experience with two such cases of comminuted avulsion fractures of the proximal fibular with posterolateral ligament ruptures surgically fixated with a locking compression hook plate and non absorbable sutures.
Figures and Tables
Fig. 1
Left knee antero-posterior and lateral view show a comminuted avulsion fracture of the fibular head.

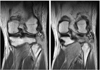

Fig. 4
Intraoperative photograph shows the avulsion fracture of the fibular head and lateral collateral ligament injury. The blue: comminuted avulsion fracture of the proximal fibula. The red: avulsed and stretched lateral collateral ligament. The yellow: common peroneal nerve.

Fig. 5
The lateral collateral ligament was sutured using a non-absorbable suture with Baseball whipstitch technique. The blue: comminuted avulsion fracture of the proximal fibula. The red: avulsed and stretched lateral collateral ligament. The yellow: common peroneal nerve. The white: non absorbable suture (#5 ethibond).


References
1. Baker CL Jr, Norwood LA, Hughston JC. Acute posterolateral rotatory instability of the knee. J Bone Joint Surg Am. 1983. 65:614–618.

2. Bottomley NJ, Williams A, Birch R, Noorani A, Lewis A, Lavelle J. Beware the fibular head avulsion fracture: the anatomical pattern of posterolateral corner injury and its relation to the common peroneal nerve. J Bone Joint Surg Br. 2006. 88:252.
3. Gautier E, Sommer C. Guidelines for the clinical application of the LCP. Injury. 2003. 34:Suppl 2. B63–B76.
4. Huang GS, Yu JS, Munshi M, et al. Avulsion fracture of the head of the fibula (the "arcuate" sign): MR imaging findings predictive of injuries to the posterolateral ligaments and posterior cruciate ligament. AJR Am J Roentgenol. 2003. 180:381–387.
5. Hughston JC, Andrews JR, Cross MJ, Moschi A. Classification of knee ligament instabilities. Part II. The lateral compartment. J Bone Joint Surg Am. 1976. 58:173–179.
6. Juhng SK, Lee JK, Choi SS, Yoon KH, Roh BS, Won JJ. MR evaluation of the "arcuate" sign of posterolateral knee instability. AJR Am J Roentgenol. 2002. 178:583–588.
7. Niemeyer P, Südkamp NP. Principles and clinical application of the locking compression plate (LCP). Acta Chir Orthop Traumatol Cech. 2006. 73:221–228.
8. Oh HK, Kim JH, Lee CS, Singh PK, Wang KH, Nha KW. Isolated avulsion fracture of the fibular head: a new fixation technique using a suture anchor. Orthopedics. 2011. 34:100–104.
9. Stoffel K, Dieter U, Stachowiak G, Gächter A, Kuster MS. Biomechanical testing of the LCP-how can stability in locked internal fixators be controlled? Injury. 2003. 34:Suppl 2. B11–B19.
 XML Download
XML Download