

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To acquire anatomical data for the normal pelvic bone structure using three-dimensional computed tomography (3D CT) and to propose the most appropriate angle and screw length for safe screw insertion during symphysis pubis plating.
Materials and Methods
We performed 3D CT analysis in 52 patients who required plating and selected a medial and lateral insertion point between the symphysis pubis and the pubic tubercle. Using a three-dimensional medical image analysis program, we evaluated the appropriate screw length, sagittal angle, and oblique angle at each point in this cohort.
Results
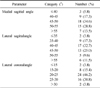
At the medial point, the sagittal angle was determined to be 49.1° with an average screw length of 49.4 mm. At the lateral point, we calculated an average screw length of 49.1 mm, oblique angle of 23.2°, and sagittal angle of 45.7°. The screw length was longer in men than in women (4.6 mm and 7.3 mm, respectively) at the medial and lateral point.
Figures and Tables
Fig. 1
(A) Initial pelvis antero-posterior image of a 47-year-old male showing pelvic ring injury with sacroiliac joint fracture and dislocation and symphysis pubis diastasis.
(B) Postoperative radiograph demonstrating the protruded screw at left pubis.
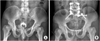
Fig. 2
A schematic picture showing screw fixation of symphysis pubis. A mark (*) of indicates pubic tubercle. Medial insertion point is the bisecting point between pubic tubercle and symphysis pubis; and lateral insertion point is just lateral to pubic tubercle.

Fig. 3
With 3-dimensional reconstruction image, measuring sagittal angle length at the medial insertion.
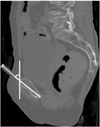
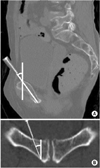
Fig. 4
With 3-dimensional reconstruction image, measuring.
(A) Sagittal angle and length.
(B) Oblique angle at the lateral position.

References
1. Bagchi K, Uhl RL. Fixation of pubic symphyseal disruptions: one or two plates? Orthopedics. 2009. 32:427.

2. Kim JJ, Kim JW, Chang JS. Clinical outcome of AO Type C pelvic ring injury. J Korean Orthop Assoc. 2005. 40:181–187.
3. MacAvoy MC, McClellan RT, Goodman SB, et al. Stability of open-book pelvic fractures using a new biomechanical model of single-limb stance. J Orthop Trauma. 1997. 11:590–593.
4. Matta JM, Saucedo T. Internal fixation of pelvic ring fractures. Clin Orthop Relat Res. 1989. (242):83–97.
5. Meissner A, Fell M, Wilk R, Boenick U, Rahmanzadeh R. Comparison of internal fixation methods for the symphysis in multi-directional dynamic gait simulation. Unfallchirurg. 1998. 101:18–25.
6. Park SE, Kim YY, Ji JH, Han CW, Kim WY. Testicular necrosis after ilioinguinal approach for pelvic nonunion: a case report. J Korean Fract Soc. 2006. 19:490–493.
7. Ponson KJ, Hoek van Dijke GA, Joosse P, Snijders CJ, Agnew SG. Improvement of external fixator performance in type C pelvic ring injuries by plating of the pubic symphysis: an experimental study on 12 external fixators. J Trauma. 2002. 53:907–912.
8. Ponsen KJ, Joosse P, Schigt A, Goslings JC, Luitse JS. Internal fracture fixation using the Stoppa approach in pelvic ring and acetabular fractures: technical aspects and operative results. J Trauma. 2006. 61:662–667.
9. Rommens PM, Hessmann MH. Staged reconstruction of pelvic ring disruption: differences in morbidity, mortality, radiologic results, and functional outcomes between B1, B2/B3, and C-type lesions. J Orthop Trauma. 2002. 16:92–98.
10. Sagi HC, Ordway NR, DiPasquale T. Biomechanical analysis of fixation for vertically unstable sacroiliac dislocations with iliosacral screws and symphyseal plating. J Orthop Trauma. 2004. 18:138–143.
11. Sagi HC, Papp S. Comparative radiographic and clinical outcome of two-hole and multi-hole symphyseal plating. J Orthop Trauma. 2008. 22:373–378.
12. Simonian PT, Routt ML Jr, Harrington RM, Tencer AF. Box plate fixation of the symphysis pubis: biomechanical evaluation of a new technique. J Orthop Trauma. 1994. 8:483–489.
13. Simonian PT, Schwappach JR, Routt ML Jr, Agnew SG, Harrington RM, Tencer AF. Evaluation of new plate designs for symphysis pubis internal fixation. J Trauma. 1996. 41:498–502.
14. Stocks GW, Gabel GT, Noble PC, Hanson GW, Tullos HS. Anterior and posterior internal fixation of vertical shear fractures of the pelvis. J Orthop Res. 1991. 9:237–245.
15. Taller S, Srám J, Lukás R, Krivohlávek M. Surgical treatment of pelvic ring and acetabular fractures using the Stoppa approach. Acta Chir Orthop Traumatol Cech. 2010. 77:93–98.
16. Varga E, Hearn T, Powell J, Tile M. Effects of method of internal fixation of symphyseal disruptions on stability of the pelvic ring. Injury. 1995. 26:75–80.
17. Webb LX, Gristina AG, Wilson JR, Rhyne AL, Meredith JH, Hansen ST Jr. Two-hole plate fixation for traumatic symphysis pubis diastasis. J Trauma. 1988. 28:813–817.
 XML Download
XML Download