

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
In the treatment of intertrochanteric fractures, most of intramedullary nailings are performed on a fracture table in supine position. In supine position, however, soft tissue mass of the patients and drapes make it difficult to access to the piriformis fossa and to straighten the trajectory of reamer and nail insertion. To resolve these problems, we have treated twenty intertrochanteric fractures in lateral position on the general operation table with IM nail. Adjustment of the position of lag screw in femoral head was done with the technique that overlaps the shadows of the femoral head, nail and targeting guide in the lateral view. Because the entire injured limb can be moved readily, it was easy to reduce fracture and to convert to open procedure. In cases likely that the fracture table is unavailable in which patients are obese, have short stature or are amputated, and that open procedure is strongly likelihood, lateral position will be helpful technique in the treatment of intertrochanteric fractures with IM nail.
Figures and Tables
Fig. 1
For anteroposterior view, C-arm is rotated under a table. Rolled sheets are placed under knee and ankle of the patient for reduction of fracture.

Fig. 2
Lateral view of proximal femur.
(A) The shadows of femoral head, nail and targeting guide overlap.
(B) Diagram of C-arm view.
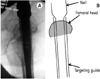
Fig. 3
Adjustment of the anteversion of lag screw
(A) Simulation with saw bones shows that the rotation of targeting guide determines position of lag screw in the femoral head.
(B) Corresponding C-arm views show shadows of 3-components, in which contours of targeting guides are outlined with solid line.

References
1. Carr JB. The anterior and medial reduction of intertrochanteric fractures: a simple method to obtain a stable reduction. J Orthop Trauma. 2007. 21:485–489.

2. Haidukewych GJ. Intertrochanteric fractures: ten tips to improve results. J Bone Joint Surg Am. 2009. 91:712–719.
3. Joseph TN, Chen AL, Kummer FJ, Koval KJ. The effect of posterior sag on the fixation stability of intertrochanteric hip fractures. J Trauma. 2002. 52:544–547.
4. Koval KJ, Zuckerman JD. Bucholz RW, Heckman JD, editors. Intertrochanter fractures. Rockwood and Green's fractures in adults. 2001. 7th ed. Philadelphia: Lippincott, Williams and Wilkins;1635–1663.
5. May JM, Chacha PB. Displacements of trochanteric fractures and their influence on reduction. J Bone Joint Surg Br. 1968. 50:318–323.
6. Oh JK, Hwang JH. Osteoporotic pertrochanteric fracture: IM nailing. J Korean Fract Soc. 2009. 22:56–65.
7. Ostrum RF, Marcantonio A, Marburger R. A critical analysis of the eccentric starting point for trochanteric intramedullary femoral nailing. J Orthop Trauma. 2005. 19:681–686.
8. Ozsoy MH, Basarir K, Bayramoglu A, Erdemli B, Tuccar E, Eksioglu MF. Risk of superior gluteal nerve and gluteus medius muscle injury during femoral nail insertion. J Bone Joint Surg Am. 2007. 89:829–834.
9. Sirkin MS, Behrens F, McCracken K, Aurori K, Aurori B, Schenk R. Femoral nailing without a fracture table. Clin Orthop Relat Res. 1996. 332:119–125.
10. Stephen DJ, Kreder HJ, Schemitsch EH, Conlan LB, Wild L, McKee MD. Femoral intramedullary nailing: comparison of fracture-table and manual traction. a prospective, randomized study. J Bone Joint Surg Am. 2002. 84:1514–1521.
 XML Download
XML Download