

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate radiological and clinical results of the antegrade intramedullary prebent K-wire fixation for the 5th metacarpal neck fracture.
Materials and Methods
Between January, 2006 and December, 2009, 31 patients with displaced neck fracture of the fifth metacarpal who received antegrade intramedullary prebent K-wire fixation were included in this study. Radiological and clinical outcome evaluations were performed.
Results
All the fractures were completely united. In the oblique radiographs, the average of preoperative angulation was corrected from 38.9° to 4.4°. The average difference between postoperative and final follow-up was 1.2°. Clinical outcomes were satisfactory except for one patient who had sustained ulnar nerve dorsal branch injury during surgery.
Figures and Tables

 | Fig. 2The wire is inserted through the ulnar cortex of the little finger metacarpal base, after 5 mm incision.
|
 | Fig. 4Prebent tip of the wire is secured at the subchondral bone of the metacarpal head after closed reduction under the C-arm.
|
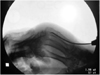
 | Fig. 5A 46-year old man sustains a 5th metacarpal neck fracture with 35° angulation deformity in oblique radiograph.
|





References
1. Ali A, Hamman J, Mass DP. The biomechanical effects of angulated boxer's fractures. J Hand Surg Am. 1999. 24:835–844.

2. Braakman M, Oderwald EE, Haentjens MH. Functional taping of fractures of the 5th metacarpal results in a quicker recovery. Injury. 1998. 29:5–9.
3. Choi SJ, Chang SK. Teatment method of the metacarpal bone fractures with retrograde percutaneous intramedullary K-wire fixation to decrease the injury of extensor tendon. J Korean Soc Surg Hand. 2004. 9:117–122.
4. Ford DJ, Ali MS, Steel WM. Fractures of the fifth metacarpal neck: is reduction or immobilisation necessary? J Hand Surg Br. 1989. 14:165–167.
5. Foucher G. "Bouquet" osteosynthesis in metacarpal neck fractures: a series of 66 patients. J Hand Surg Am. 1995. 20:S86–S90.
6. Foucher G, Chemorin C, Sibilly A. A new technic of osteosynthesis in fractures of the distal 3d of the 5th metacarpus. Nouv Presse Med. 1976. 5:1139–1140.
7. Hunter JM, Cowen NJ. Fifth metacarpal fractures in a compensation clinic population. A report on one hundred and thirty-three cases. J Bone Joint Surg Am. 1970. 52:1159–1165.
8. Jahss SA. Fracture of the metacarpals: a new method of reduction and immobilization. J Bone Joint Surg Am. 1938. 20:178–186.
9. Kim BS, Cho SD, Cho YS, et al. Operative treatment of metacarpal shaft fracture. J Korean Soc Fract. 1999. 12:720–726.
10. Kim MH, Yoo MJ, Kim JP, Lee JH, Lee JW. Bouquet pin intramedullary nail technique of the 5th metacarpal neck fractures. J Korean Fract Soc. 2007. 20:64–69.
11. Lamraski G, Monsaert A, De Maeseneer M, Haentjens P. Reliability and validity of plain radiographs to assess angulation of small finger metacarpal neck fractures: human cadaveric study. J Orthop Res. 2006. 24:37–45.
12. Leung YL, Beredjiklian PK, Monaghan BA, Bozentka DJ. Radiographic assessment of small finger metacarpal neck fractures. J Hand Surg Am. 2002. 27:443–448.
13. Manueddu CA, Della Santa D. Fasciculated intramedullary pinning of metacarpal fractures. J Hand Surg Br. 1996. 21:230–236.
14. McKerrell J, Bowen V, Johnston G, Zondervan J. Boxer's fractures--conservative or operative management. J Trauma. 1987. 27:486–490.
15. Paul AS, Kurdy N, Kay PR. Fixation of closed metacarpal shaft fractures. Transverse K-wires in 22 cases. Acta Orthop Scand. 1994. 65:427–429.
16. Steel WM. Barton NJ, editor. Articular fractures. Fractures of the hand and wrist. 1988. New York: Churchill Livingstone;55–73.
17. Theeuwen GA, Lemmens JA, van Niekerk JL. Conservative treatment of boxer's fracture: a retrospective analysis. Injury. 1991. 22:394–396.
18. Wong TC, Ip FK, Yeung SH. Comparison between percutaneous transverse fixation and intramedullary K-wires in treating closed fractures of the metacarpal neck of the little finger. J Hand Surg Br. 2006. 31:61–65.
 XML Download
XML Download