

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To investigate the relationship between the greenstick laminar fractures and the dural tear in low lumbar burst fractures and their optimal treatment.
Materials and Methods
We enrolled 51 patients (52 cases) who had been diagnosed with low lumbar burst fracture from June 2003 to May 2007. The average age was 39 years (range, 22 to 58), 30 male patients (58.8%), and 21 female patients (41.2%). Average follow-up periods was 19 months (range, 11 to 45). Lumbar CT scan were taken 1 mm slices in precision for all patients. We judged it incomplete fracture if lumbar CT scans show loss of cortical continuity over 3 slices if there is an aggrement of two among one radiologist and two orthopaedic surgeons reached a consensus. Dural tear and entrapment of nerve root were confirmed intraoperatively by the senior surgeon.
Results
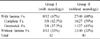
In 52 burst fractures, complete lamina fractures occurred in 21 cases and there were green stick laminar fractures in 14 cases. Neurologic defect has been found in 12 cases, 5 (63%) from complete laminar fractures and 3 (37%) from green stick laminar fractures. Dural tears has been detected in 9 cases (26%), 4 (19%) from complete laminar fractures and 5 (36%) from green stick laminar fractures.
Figures and Tables
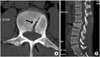 | Fig. 1Axial (A) and sagittal (B) CT scans show L3 burst fracture with green stick laminar fracture (arrow) in 22 year-old man who fell from height. Initial Frankel grade was D.
|
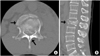 | Fig. 2Axial (A) and sagittal (B) CT scans show L2 burst fracture with greenstick laminar fracture and 70% of spinal canal occlusion (arrow) in 49 year-old man who had motor vehicle accident. Initial Frankel grade was C.
|


References
1. Andreychik DA, Alander DH, Senica KM, Stauffer ES. Burst fractures of the second through fifth lumbar vertebrae. Clinical and radiographic results. J Bone Joint Surg Am. 1996. 78:1156–1166.

2. Aydinli U, Karaeminoğullari O, Tişkaya K, Oztürk C. Dural tears in lumbar burst fractures with greenstick lamina fractures. Spine (Phila Pa 1976). 2001. 26:E410–E415.
3. Bradford DS, McBride GG. Surgical management of thoracolumbar spine fractures with incomplete neurologic deficits. Clin Orthop Relat Res. 1987. 218:201–216.
4. Brant-Zawadzki M, Jeffrey RB Jr, Minagi H, Pitts LH. High resolution CT of thoracolumbar fractures. AJR Am J Roentgenol. 1982. 138:699–704.
5. Bridwell KH. Floman Y, Farcy JPC, Argenson C, editors. Low lumbar (L3-L4-L5) burst fractures. Thoracolumbar spine fracture. 1993. New York: Raven;223–234.
6. Cammisa FP Jr, Eismont FJ, Green BA. Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am. 1989. 71:1044–1052.
7. Denis F. Spinal instability as defined by the three-column spine concept in acute spinal trauma. Clin Orthop Relat Res. 1984. 189:65–67.
8. Denis F, Burkus JK. Diagnosis and treatment of cauda equina entrapment in the vertical lamina fracture of lumbar burst fractures. Spine (Phila Pa 1976). 1991. 16:8 Suppl. S433–S439.
9. Keene JS, Fischer SP, Drummond DS. The neurological consequences of post traumatic impingement. Presented at the 52nd Annual Meeting of American Academy of Orthopaedic Surgeons. 1985; Las Vegas, Nevada.
10. Kim YM, Kim DS, Choi ES, et al. Bone & soft tissue injuries diagnosed by magnetic resonance imaging in thoracolumbar fractures. J Korean Fract Soc. 2004. 17:184–190.
11. McAfee PC, Yuan HA, Fredrickson BE, Lubicky JP. The value of computed tomography in thoracolumbar fractures. An analysis of one hundred consecutive cases and a new classification. J Bone Joint Surg Am. 1983. 65:461–473.
12. Miller CA, Dewey RC, Hunt WE. Impaction fracture of the lumbar vertebrae with dural tear. J Neurosurg. 1980. 53:765–771.
13. Ozturk C, Ersozlu S, Aydinli U. Importance of greenstick lamina fractures in low lumbar burst fractures. Int Orthop. 2006. 30:295–298.
14. Park YS, Son KH, Park KC, Sung IH, Cho JL. Relevancy of posterior column injury and dural tear in unstable burst fracture. J Korean Fract Soc. 2005. 18:65–68.
15. Pau A, Silvestro C, Carta F. Can lacerations of the thoraco-lumbar dura be predicted on the basis of radiological patterns of the spinal fractures? Acta Neurochir (Wien). 1994. 129:186–187.
16. Pickett J, Blumenkopf B. Dural lacerations and thoracolumbar fractures. J Spinal Disord. 1989. 2:99–103.
17. Trafton PG, Boyd CA Jr. Computed tomography of thoracic and lumbar spine injuries. J Trauma. 1984. 24:506–515.
 XML Download
XML Download