

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
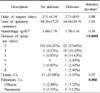
To evaluate the incidence, risk factors and prognosis of delirium in elderly patients with intertrochanteric fractures of femur.
Materials and Methods
162 patients who underwent operation for intertrochanteric fracture of femur from July 2005 to January 2007 were reviewed retrospectively. Delirium was diagnosed by using Confusion Assessment Method (CAM). Medical records were reviewed for the information of the patients, Gross motor function classification of Palisano et al. was used for the evaluation of ambulatory status. Univariate analysis and multivariate analysis were done to find out the risk factors.
Results
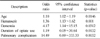
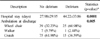
2 cases out of 162 (1.2%) met the criteria of delirium at admission, and 39 cases (24.1%) after surgery. Univariate analysis and multivariate analysis identified age, hematocrit, dementia, the duration of opiate use, and pulmonary complication as risk factors. Hospital stay was longer and postoperative ambulatory status was worse in the patients with delirium.
Figures and Tables
Table 1
Confusion assessment method (CAM). The diagnosis of delirium by CAM requires the presence of features 1 and 2 and either 3 or 4

![]()




References
1. Bergström U, Jonsson H, Gustafson Y, Pettersson U, Stenlund H, Svensson O. The hip fracture incidence curve is shifting to the right. Acta Orthop. 2009. 80:520–524.

2. Björkelund KB, Hommel A, Thorngren KG, Gustafson L, Larsson S, Lundberg D. Reducing delirium in elderly patients with hip fracture: a multi-factorial intervention study. Acta Anaesthesiol Scand. 2010. 54:678–688.
3. Cole MG, Primeau FJ. Prognosis of delirium in elderly hospital patients. CMAJ. 1993. 149:41–46.
4. Dasgupta M, Dumbrell AC. Preoperative risk assessment for delirium after noncardiac surgery: a systematic review. J Am Geriatr Soc. 2006. 54:1578–1589.
5. Furlaneto ME, Garcez-Leme LE. Delirium in elderly individuals with hip fracture: causes, incidence, prevalence, and risk factors. Clinics (Sao Paulo). 2006. 61:35–40.
6. George J, Bleasdale S, Singleton SJ. Causes and prognosis of delirium in elderly patients admitted to a district general hospital. Age Ageing. 1997. 26:423–427.
7. Inouye SK. Predisposing and precipitating factors for delirium in hospitalized older patients. Dement Geriatr Cogn Disord. 1999. 10:393–400.
8. Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999. 340:669–676.
9. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990. 113:941–948.
10. Juliebø V, Bjøro K, Krogseth M, Skovlund E, Ranhoff AH, Wyller TB. Risk factors for preoperative and postoperative delirium in elderly patients with hip fracture. J Am Geriatr Soc. 2009. 57:1354–1361.
11. Kim KH, Kho DH, Shin JY, Choi JY, Kim ES, Kim DH. Risk factors of postoperative delirium in elderly patients with hip fractures. J Korean Fract Soc. 2008. 21:189–194.
12. Marcantonio ER, Flacker JM, Wright RJ, Resnick NM. Reducing delirium after hip fracture: a randomized trial. J Am Geriatr Soc. 2001. 49:516–522.
13. McNicoll L, Fitzgibbons PG. Optimal hip fracture management in high-risk frail older adults. Med Health R I. 2009. 92:250–252.
14. Morrison RS, Magaziner J, Gilbert M, et al. Relationship between pain and opioid analgesics on the development of delirium following hip fracture. J Gerontol A Biol Sci Med Sci. 2003. 58:76–81.
15. Palisano RJ, Rosenbaum P, Bartlett D, Livingston MH. Content validity of the expanded and revised gross motor function classification system. Dev Med Child Neurol. 2008. 50:744–750.
16. Pedersen SJ, Borgbjerg FM, Schousboe B, et al. A comprehensive hip fracture program reduces complication rates and mortality. J Am Geriatr Soc. 2008. 56:1831–1838.
17. Robertson BD, Robertson TJ. Postoperative delirium after hip fracture. J Bone Joint Surg Am. 2006. 88:2060–2068.
18. Saxena S, Lawley D. Delirium in the elderly: a clinical review. Postgrad Med J. 2009. 85:405–413.
19. Song WS, Choi JC, Lee YS, et al. The risk factors of delirium in elderly patients with hip fracture: a prospective study. J Korean Hip Soc. 2008. 20:293–298.
20. Trzepacz PT. Delirium. Advances in diagnosis, pathophysiology, and treatment. Psychiatr Clin North Am. 1996. 19:429–448.
21. van der Mast RC. Pathophysiology of delirium. J Geriatr Psychiatry Neurol. 1998. 11:138–145.
 XML Download
XML Download