

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To study clinical results and complications in the treatment of infected nonunion of the tibia according to location of nonunion and reconstruction for soft tissue defect.
Materials and Methods
36 cases of tibia infected nonunion which were treated with the llizarov included in this study. There were proximal 1/3 in 14, middle 1/3 in 10, and distal 1/3 in 11 cases. Coverage of the soft tissue were treated with the free flap in 8 cases as classified group A and non-free flap in 17 cases classified group B. We evaluated the healing index, complications and comparing the results of each treatment by the Paley method.
Results
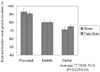
Bone union was achieved in all cases. The proximal nonunion showed better results than those in the middle and distal area; average healing index: 35.6 days/cm (p=0.038), bone results: 92.9% (p=0.025), functional result: 90.5% (p=0.03). Group B showed significantly better results as it showed average healing index: 30.3 days/cm (p=0.015), bone results: 85.7% (p=0.025), functional results: 90.5% (p=0.015).
Figures and Tables
 | Fig. 1The 67 year-old male sustained comminuted open fracture of the right distal tibia and fibula (Gustilo III-c type) with soft tissue defect by traffic accident. External fixation was done, but delayed soft tissue coverage, then developed infected nonunion with chronic osteomyelitis according to Paley classification at postoperative 5 months.
(A) Roentgenograms showed nonunion tibia with soft tissue defect.
(B) The free flap of latissimus dorsi applied to soft tissue defect site.
(C) After radical excision of all necrotic tissue, applied bifocal Ilizarov frame with acute shortening of 6cm in length and inserted vancomycin beads.
(D) Follow-up study at eight months after operation with Ilizarov technique showed consolidation of regenerates and union of docking site.
(E) Roentgenograms fifteen months after operation showed excellent bone and functional result.
|
 | Fig. 2The 27 year-old male sustained comminuted open fracture of the right tibia and fibula (Gustilo III-c type) with soft tissue defect by traffic accident. We couldn't check posterior tibial artery pulsation in ankle area. Closed reduction and external fixation was done, because unstable vital condition. Then developed infected nonunion with chronic osteomyelitis according to Paley classification at postoperative 3 months.
(A) Roentgenograms showed comminuted tibia and fibular fracture.
(B) Closed reduction and external fixation was done in emergency operation.
(C) Then developed infected nonunion with soft tissue defect after 3 months.
(D) After radical excision of all necrotic tissue, applied bifocal Ilizarov frame with acute shortening of 5 cm in length.
(E) Follow-up study at 10 months after operation with Ilizarov technique showed consolidation of regenerates and union of docking site.
(F) Roentgenograms 16 months after operation showed excellent bone result and good functional result.
|



References
1. Alt V, Meeder PJ, Seligson D, Schad A, Atienza C Jr. The proximal tibia metaphysic: a reliable donor site for bone grafting? Clin Orthop Relat Res. 2003. 414:315–321.
2. Aronson J, Johnson E, Harp JH. Local bone transportation for treatment of intercalary defects by the Ilizarov technique. Biomechanical and clinical considerations. Clin Orthop Relat Res. 1989. 243:71–79.
3. Cattaneo R, Catagni M, Johnson EE. The treatment of infected nonunions and segmental defects of the tibia by the methods of Ilizarov. Clin Orthop Relat Res. 1992. 280:143–152.

4. DeCoster TA, Gehlert RJ, Mikola EA, Pirela-Cruz MA. Management of posttraumatic segmental bone defects. J Am Acad Orthop Surg. 2004. 12:28–38.
5. Dendrinos GK, Kontos S, Lyristsis E. Use of the Ilizarov technique for treatment of non-union of the tibia associated with infection. J Bone Joint Surg Am. 1995. 77:835–846.
6. Duman H, Sengezer M, Celikoz B, Turegun M, Isik S. Lower extremity salvage using a free flap associated with the Ilizarov method in patients with massive combat injuries. Ann Plast Surg. 2001. 46:108–112.
7. Freeland AE, Mutz SB. Posterior bone grafting for infected ununited fractures of the tibia. J Bone Joint Surg Am. 1976. 58:653–657.
8. Gordon L, Chiu EJ. Treatment of infected nonunions and segmental defects of the tibia with staged microvascular muscle transplantation and bone-grafting. J Bone Joint Surg Am. 1988. 70:377–386.
9. Gustilo RB, Merkow RL, Templeman D. The management of open fractures. J Bone Joint Surg Am. 1990. 72:299–304.
10. Hahn SB, Park YW, Park HW, Kim HW, Kim BH. Comparison of treating tibial nonunion with bone and soft tissue defect: Ilizarov only versus free flap and Ilizarov. J Korean Orthop Assoc. 2002. 37:754–758.
11. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues. Part II. The influence of rate and frequency of distraction. Clin Orthop Relat Res. 1989. 239:263–285.
12. Jupiter JB, Kour AK, Palumbo MD, Yaremchuk MJ. Limb reconstruction by free-tissue transfer combined with the Ilizarov method. Plast Reconstr Surg. 1991. 88:943–954.
13. Lowenberg DW, Feibel RJ, Louie KW, Eshima I. Combined muscle flap and Ilizarov reconstruction for bone and soft tissue defects. Clin Orthop Relat Res. 1996. 332:37–51.
14. Maini L, Chadha M, Vishwanath J, Kapoor S, Mehtani A, Dhaon BK. The Ilizarov method in infected nonunion of fractures. Injury. 2000. 31:509–517.
15. Paley D. Problems, obstacles and complication of limb lengthening by the ilizarov technique. Clin Orthop Relat Res. 1990. 250:81–104.
16. Paley D, Catagni MA, Argnani F, Villa A, Bennedetti GB, Cattaneo R. Ilizarov treatment of tibial nonunions with bone loss. Clin Orthop Relat Res. 1989. 241:146–165.
17. Schöttle PB, Werner CM, Dumount CR. Two-stage reconstruction with free vascularized soft tissue transfer and conventional bone graft for infected nonunions of the tibia: 6 patients followed for 1.5 to 5 years. Acta Orthop. 2005. 76:878–883.
18. Sen C, Kocaoqlu M, Eralp L, Gulsen M, Cinar M. Bifocal compression-distraction in the acute treatment of grade III open tibia fracture with bone and soft-tissue loss: a report of 24 cases. J Orthop Trauma. 2004. 18:150–157.
19. Tukiainen E, Asko-Seljavaara S. Use of the Ilizarov technique after a free microvascular muscle flap transplantation in massive trauma of the lower leg. Clin Orthop Relat Res. 1993. 297:129–134.
 XML Download
XML Download