

 PDF
PDF ePub
ePub Citation
Citation Print
Print


It has difficulty to treat distal humeral fracture in elderly over six decades because of extensive comminution and poor bone quality. Even though the bone defects due to severe comminution could be filled with iliac bone graft, the cancellous bone portion of iliac bone is easily resorbed. So, non-union was developed frequently in open reduction and internal fixation with iliac bone graft. In order to solve this problem, we could choose total elbow arthroplasty as alternative method for repairing non-union of distal humerus. But, complications of elbow arthroplasty itself are obstacle to choose this rising method. So, we reconstructed humeral condyle with fibular inlay graft making triangular structure inside cortical shell of intercondylar bone fragments. It obtained relatively good clinical result. So, we introduce this procedure for one of treatment option for repairing non-union of comminuted distal humeral fractures.
CASE REPORT
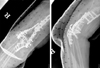
A 59 year old woman suffered severely comminuted intercondylar fracture caused by falling on her right arm outstretched (Fig. 1A). Open reduction and internal fixation using plate and screws with iliac bone graft was performed (Fig. 1B).
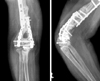
Two years later, she was still complaining of pain and limitation of movements. She had an arc of flexion of from 45° to 90°, pronation of 40° and supination of 60°, and she had another slip down injury during observation period. Radiographs show resorption of grafted bone and new fracture near proximal portion of the plate in addition to nonunion of initial fracture of the distal humerus (Fig. 2).
Operation was performed under general anesthesia with the patient in the lateral decubitus position with the shoulder at 90 degrees of abduction and the elbow at 90 degrees of flexion, over bolsters. The posterior approach was used, with sterile pneumatic tourniquet5). The ulnar nerve was identified and tagged with a vessel loop. All fixation devices which were used in previous operation were removed. The olecranon was osteotomized and flipped proximally and the distal end of the humerus was visualized directly. The trochlea and the capitellum were comminuted into three fragments. The supracondylar area of distal humerus was comminuted in a mutifragmentary manner. According to radiograph of initial trauma (Fig. 1A), this fracture type was categorized as type C3-3 according to AO/ASIF classification4), which is defined as T or Y bicondylar fracture with severe comminution on intercondylar and supracondylar area. Radiographs at the time of nonunion showed most supracondylar fragments were small and osteoporotic.
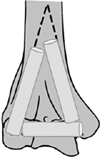
Fibular free graft was harvested at once and divided into 3 parts for reconstruction of condyles. Fibular inlay graft was made into triangular shape to fit humeral condyles. The articular surfaces were temporarily stabilized using a small bone reduction forceps and a few 1.8 mm Kirschner wires. Then the articular fragments were held in place with reconstruction plates and cortical and cancellous screw that was placed transversely from outside to inside to hold the condyles. Allo-bone confounded with cancellous bone was impacted on gap between graft and cortex. New fracture near proximal portion of the plate was reduced and fixed by plate and screws. Finally, the olecranon was reduced and fixed with two Kirshner wires, tension band wire and plate & screws. It was confirmed that all fragments were stable and the olecranon and coronoid fossa were not compromised by bone fragments or hardware (Fig. 3).
The patient was placed into long arm splint and was elevated for 48 hours. Physical therapy was begun 2 weeks postoperatively.
She felt no instability or pain on activity of daily living. One hundred and ten degrees of range of motion (120 degrees of flexion and 10 degrees of loss of extension) was achieved at 10 months after the operation (Fig. 4). Radiograph shows bony union of entire humerus (Fig. 5). The functional result was excellent according to Broberg and Morrey's functional scale at 10 months after operation2).
DISCUSSION
The internal fixation of comminuted fractures of the distal end of humerus is difficult, especially if bone is osteoporotic. McKee et al. reported that open reduction and internal fixation could be effective even in the elderly if only rigid fixation was obtained to allow early exercise7). And Ahn et al. insisted to obtain the satisfactory results in distal humeral fractures, stable fixation followed by early motion is required in most distal humeral fractures1). So, authors did open reduction and internal fixation with autologous iliac bone graft for initial treatment. But, resorption of grafted iliac bone, severe comminution and poor bone quality leaded to nonunion. So we needed salvage operation by open reduction and internal fixation with bone grafting again or total elbow arthroplasty, which are considerably challenging procedures because its own complication. We therefore hypothesized that reconstruction using free fibular inlay graft by making triangular structure could be a recommendable surgical method treating a certain case of humeral intercondylar comminuted fracture which only cortical shell remained. Although vascularized fibular graft was recommended theoretically but free non-vascularized fibular graft reported good outcome as treatment of post-traumatic bone defects3). And in this case, authors made triangular structure by dividing single fibular bone, all three block couldn't get vessel supplied.
In recent few years total elbow arthroplasty was appeared alternative method for intra-articular, comminuted distal humeral fractures for elderly6,10). But, complications of total elbow arthroplasty such as neurolysis, instability, infection, revisional surgery was remained obstacle to choose arthroplasty as primary method for fracture treatment6,8,9). Especially in nonunion, controversy was existed. So, authors devised procedure that could provide structural support by triangular shape like condyles using fibular graft with plate & screws. It achieved great radiological & functional results. We hope this procedure to become one of the options for treatment for comminuted comminuted fracture of the elbow in the elderly.



 XML Download
XML Download