

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The purpose of this study was to classify posterior malleolar fractures according to the position of fragments and to analyze radiologic features of each type.
Materials and Methods
We analyzed forty-six patients of ankle fractures involving a posterior malleolus who were treated between January 2004 and December 2007. The posterior malleolar fractures were categorized into three types (posterolateral, posteromedial, shell) based on the major fracture line. In each type, we analyzed amount of displacement, involvement of articular surface, existence of subluxation and osteochondral impacted fragments.
Results
The forty-six patients were categorized into three types: Posterolateral (PL) type (33 cases, 72%), Posteromedial (PM) type (8 cases, 17%), shell type (5 cases, 11%). Of the 8 cases with PM type, 7 cases showed displacement more than Grade II, 4 cases showed subluxation of ankle joint, and 3 cases showed osteochondral impacted fragment. Average involvement of articular surface of PM type is 35% (15~65%).
Figures and Tables
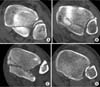 | Fig. 1Transverse CT scans showing a type of the posterior malleolar fractures.
(A) Type I fracture of the posterior malleolar, with triangular fragment involving the posterolateral corner of the tibial plafond.
(B) Type II-A fracture of the posterior malleolus with extension of the fracture line to the anterior part of the medial malleolar (anterior colliculus).
(C) Type II-B fracture of the posterior malleolar, with extension of the fracture line to the posterior colliculus.
(D) Type III fracture of the posterior malleolar, with small shell-shaped fragments at the posterior lip of the tibial plafond.
|
 | Fig. 2
(A) A 62 years old woman had a posterior malleolar fragment. The fracture line extends to the anterior part of the medial malleolar (anterior colliculus).
(B) Access between medial malleolar and the posteromedial fragment (arrow). The posteromedial fragment was fixed with buttress plate, and posterolateral fragment was fixed with cannulated screw.
|
 | Fig. 3
(A) A 65 years old woman had a trimalleolar fracture. The medial double contour is well visible (arrow). The posterior malleolar fracture line extends to the posterior colliculus.
(B) Access between achilles tendon and the peroneus tendon (arrow). The posterior malleolar was fixed with buttress plate, and impacted fragment was fixed with screw.
|


References
1. Bae SY, Sihn DH. The role of posterior malleolar frag ments in ankle pain after trimalleolar fractures. J Korean Soc Fract. 2003; 16:59–66.

2. Boggs LR. Isolated posterior malleolar fractures. Am J Emerg Med. 1986; 4:334–336.
3. Chung MY, Rhi WS, Song WC, Lee SM, Seo SD. Surgical treatment of fractures of the ankle. J Korean Orthop Assoc. 1997; 32:741–748.
4. Court-Brown CM, McBirnie J, Wilson G. Adult ankle fractures-an increasing problem? Acta Orthop Scand. 1998; 69:43–47.
5. Ebraheim NA, Mekhail AO, Haman SP. External rotation-lateral view of the ankle in the assessment of the posterior malleolus. Foot Ankle Int. 1999; 20:379–383.
6. Ebraheim NA, Wong FY. External rotation views in the diagnosis of posterior colliculus fracture of the medial malleolus. Am J Orthop. 1996; 25:380–382.
7. Haraguchi N, Haruyama H, Toga H, Kato F. Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am. 2006; 88:1085–1092.
8. Harper MC, Hardin G. Posterior malleolar fractures of the ankle associated with external rotation-abduction injuries. Results with and without internal fixation. J Bone Joint Surg Am. 1988; 70:1348–1356.
9. Jaskulka RA, Ittner G, Schedl R. Fractures of the posterior tibial margin: their role in the prognosis of malleolar fractures. J Trauma. 1989; 29:1565–1570.
10. Jeong HJ, Kim KC, Chung SW. Treatment of the posterior malleolar fracture. J Korean Soc Fract. 1998; 11:924–931.
11. Kang CN, Kim JO, Lee SB, Kang OY, Shin MS. Treatment of the posterior lip fracture of distal tibia using posteromedial approach. J Korean Soc Fract. 1995; 8:594–599.
12. Katioz H, Bombaci H, Görgec M. Treatment of trimalleolar fractures. Is osteosynthesis needed in posterior malleolar fractures measuring less than 25% of the joint surface? Acta Orthop Traumatol Turc. 2003; 37:299–303.
13. Lee CS, Suh JS, Yi JW. Comparative study for the results of ankle fracture depending on the extension of the posterior malleolus fracture. J Korean Orthop Assoc. 2007; 42:470–474.
14. McDaniel WJ, Wilson FC. Trimalleolar fractures of the ankle. An end result study. Clin Orthop Relat Res. 1977; 122:37–45.
15. Neumaier Probst E, Maas R, Meenen NM. Isolated fracture of the posterolateral tibial lip (Volkmann's triangle). Acta Radiol. 1997; 38:359–362.
16. Nugent JF, Gale BD. Isolated posterior malleolar ankle fractures. J Foot Surg. 1990; 29:80–83.
17. Scheidt KB, Stiehl JB, Skrade DA, Barnhardt T. Posterior malleolar ankle fractures: an in vitro biomechanical analysis of stability in the loaded and unloaded states. J Orthop Trauma. 1992; 6:96–101.
18. Talbot M, Steenblock TR, Cole PA. Posterolateral approach for open reduction and internal fixation of trimalleolar ankle fractures. Can J Surg. 2005; 48:487–490.
19. Weber M. Trimalleolar fractures with impaction of the posteromedial tibial plafond: implications for talar stability. Foot Ankle Int. 2004; 25:716–727.
 XML Download
XML Download