

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Galeazzi fractures in child is rare and seldom necessary of operative treatment because the result of conservative treatment is good. We present the patient who was a 11-year-old male and fell onto his both hands during a hundred-meter dash. His diagnosis was bilateral Galeazzi fractures and limited open reduction and internal fixation with Kirschner pins was initial treatment at local hospital. After 4 weeks postoperatively, Kirschner pins were removed and rehabilitating exercise was started. After 4 months postoperatively, he was transferred to our hospital due to malunion with severe angular deformities and distal radioulnar joint (DRUJ) dislocation. He was treated with corrective osteotomy. Thus, as in this case, we suggest more careful treatment and observation if conservative method of Galeazzi fracture in child is chosen and consider operative method as treatment according to age and pattern of fracture.
Figures and Tables
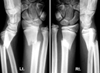 | Fig. 1Initial radiographs after the trauma showed bilateral distal radius fractures and bilateral distal radioulnar joint dislocations.
|

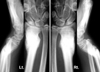
 | Fig. 3Radiographs taken at 4 weeks postoperatively after removal of K-wire and cast showed callus formation of fractures of distal radius, but showed angulation of distal radius and volar subluxation of ulnar head.
|
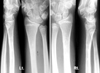
 | Fig. 4Radiographs and photographs taken at the presentation to our hospital 4 months after trauma. Radiographs showed 40 degree-angulated distal radius and dorsal dislocation of ulnar head.
|

 | Fig. 6Radiographs after corrective osteotomy and temporary K-wire fixation of distal radioulnar joint showed correction of angular deformity and reduction of ulnar head.
|
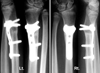 | Fig. 7Radiographs taken at 7 months after corrective osteotomy showed well-healed distal radial osteotomy site and reduced distal radioulnar joint.
|

References
1. Campbell RM Jr. Operative treatment of fractures and dislocations of the hand and wrist region in children. Orthop Clin North Am. 1990; 21:217–243.

2. Green NE, Swiontkowski MF. Galeazzi fractures. In : Browner BD, Jupiter JB, Levine AM, Trafton PG, editors. Skeletal Trauma in Children. 3rd ed. Philadelphia: WB Saunders Ins;2003. p. 229–234.
3. Herring JA. Fractures of the forearm. In : Hering HA, editor. Tachdjian's Pediatric Orthopaedics. 3rd ed. Philadelphia: WB Saunders Ins;2002. p. 2218–2246.
4. Mikić ZD. Galeazzi fracture-dislocations. J Bone Joint Surg Am. 1975; 57:1071–1080.
5. Mino DE, Palmer AK, Levinsohn EM. The role of radiography and computerised tomography in the diagnosis of subluxation and dislocation of the distal radioulnar joint. J Hand Surg Am. 1983; 8:23–31.
6. Reckling FW. Unstable fracture-dislocations of the forearm (Monteggia and Galeazzi Lesions). J Bone Joint Surg Am. 1982; 64:857–863.
7. Walsh HP, McLaren CA, Owen R. Galeazzi fractures in children. J Bone Joint Surg Br. 1987; 69:730–733.
 XML Download
XML Download