

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate the usefullness of the percutaneous reduction technique with K-wire that could reduce the displaced posterolateral fracture fragment which persisted even after an anatomical reduction of the lateral malleolar fracture.
Materials and Methods
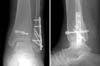
From January 2004 to December 2006, we reviewed 72 patients who underwent surgical treatment for their trimalleolar fractures. We estimated the clinical and radiological results of 5 cases treated by percutaneous reduction technique with K-wire when more than the distal tibial articular step-off was left after reduction of the lateral malleolar fracture. The method of reduction starts with temporary fixation of lateral malleolar fracture followed by checking ankle radiographic image to confirm the accuracy of reduction. In case of incomplete reduction of the posterior fragment, a K-wire is inserted into the posterior fragment and pushed downward to the ankle joint level, and then lag screws were inserted.
Results
The average articular involvement by the posterolateral fracture fragment was 30.2%. The average step-off after reduction of the lateral malleolar fracture was 3.7 mm. At the final follow up, step-off was less than 2 mm in all cases. In clinical results by Baird and Jackson score, 3 out of 5 cases were excellent, other 2 were good.
Figures and Tables

 | Fig. 2Percutaneous K-wire location is confirmed by C-arm image. Post-reduction image (A) is taken by C-arm image intensifier and the schematic image is shown (B).
|




References
1. Baird RA, Jackson ST. Fractures of the distal part of the fibula associated disruption of the deltoid ligament. Treatment without repair of the deltoid ligament. J Bone Joint Surg Am. 1987; 69:1346–1352.
2. Boggs LR. Isolated posterior malleolar fractures. Am J Emerg Med. 1986; 4:334–336.

3. Court-Brown CM, McBirnie J, Wilson G. Adult ankle fractures--an increasing problem? Acta Orthop Scand. 1998; 69:43–47.
4. De Vries JS, Wijgman AJ, Sierevelt IN, Schaap GR. Long-term results of ankle fractures with a posterior malleolar fragment. J Foot Ankle Surg. 2005; 44:211–217.
5. Haraguchi N, Haruyama H, Toga H, Kato F. Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am. 2006; 88:1085–1092.
6. Harper MC, Hardin G. Posterior malleolar fracture of the ankle associated with external rotation-abduction injuries. Results with and without internal fixation. J Bone Joint Surg Am. 1988; 70:1348–1356.
7. Jaskulka RA, Ittner G, Schedl R. Fractures of the posterior tibial margin: their role in the prognosis of malleolar fractures. J Trauma. 1989; 29:1565–1570.
8. Jeong HJ, Kin CK, Chung SW. Treatment of the posterior malleolar fracture. J Korean Soc Fract. 1998; 11:924–931.
9. Kim SJ, Choi IY, Ahn TK. A clinical study of the trimalleolar fractures of the ankle. J Korean Soc Fract. 1989; 2:145–154.
10. Lee CS, Suh JS, Yi JW. Comparative study for th results of ankle fracture depending on the extension of the posterior malleolus Fracture. J Korean Orthop Assoc. 2007; 42:470–474.
11. McDaniel WJ, Wilson FC. Trimalleolar fractures of the ankle. An end result study. Clin Orthop Relat Res. 1977; (122):37–45.
12. Michelson JD. Fractures about the ankle. J Bone Joint Surg Am. 1995; 77:142–152.
13. Neumaier Probst E, Maas R, Meenen NM. Isolated fracture of the posterolateral tibial lip (Volkmann's triangle). Acta Radiol. 1997; 38:359–362.
14. Nugent JF, Gale BD. Isolated posterior malleolar ankle fractures. J Foot Surg. 1990; 29:80–83.
15. Strenge KB, Indusuyi OB. Technique tip: percutaneus screw fixation of posterior malleolar fractures. Foot ankle Int. 2006; 27:650–652.
16. Weber M. Trimalleolar fractures with impaction of the posteromedial tibial plafond: implications for talar stability. Foot Ankle Int. 2004; 25:716–727.
 XML Download
XML Download