

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Injury to the interphalangeal (IP) joint of the great toe is relatively rare compared with injury to the meta-tarsophalangeal (MP) joint, and is easily reducible by closed methods2). However, dislocations of the IP joint of the great toe that are irreducible are very rare, having been reported only in about 40 cases1,3,4,5,6,8,10) since Muller6) first described the injury in 1944. Possible mechanism of the injury is a hyperextension force directed on the IP joint during sports activities5) and invagination of the plantar plate or the sesamoid bone into the IP joint, which prevents reduction. To our knowledge, however, dislocations of the IP joint of the great toe that were irreducible because of lateral collateral ligament entrapment, not invagination of the plantar plate or the sesamoid bone, have not been reported by any english literature. We report a 29-year-old ballet dancer who sustained an irreducible dislocation of the IP joint of the great toe owing to lateral collateral ligament entrapment.
CASE REPORT
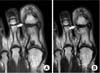
A 29-year-old female ballet dancer was brought to the emergency room of our clinics for pain in the right IP joint of the great toe. The injury occurred when the patient practiced rapid turning, using only the right great toe to support her entire weight. On physical examination, the right IP joint of the great toe showed swelling and tenderness. Tenderness was particularly severe around the lateral side of the IP joint. No deformity was observed, but the patient complained of severe pain during passive motions of the IP joint. Simple radiographs revealed a widening of the joint space and a mediodorsal dislocation of the distal phalanx, but the sesamoid bone of the plantar side was in its normal position (Fig. 1). Closed reduction was attempted under regional anesthesia, but without success. Preoperative magnetic resonance (MR) images presented complete discontinuity of the lateral collateral ligament and entrapment of the distal part of the ruptured ligament into the IP joint. Although the medial collateral ligament was intact, a medial dislocation of the distal phalanx led to bulging contour (Fig. 2). The plantar plate and the sesamoid bone were in normal positions. With a dorsolateral incision, we observed the ruptured the lateral collateral ligament and its entrapment into the joint. The plantar plate was found intact. The entrapped ligament was reduced to its original position and repaired with nonabsorbable materials. The k-wire was used for fixation of the IP joint of the great toe (Fig. 3). At four weeks after operation, the k-wire was removed and active exercises and ambulation were allowed with a wooden-soled shoe (Fig. 4). After three months, the patient began ballet dance. At six months after operation, 40 degrees of dorsiflexion and full extension were possible, while the contralateral side showed 60 degrees of dorsiflexion and full extension.
DISCUSSION
The IP joint of the great toe has a very simple anatomical structure with a high level of stability. Dislocations of the IP joint with the inherent stability are found rare. They usually occur when the joint is forced into hyperextension5) and are easily reducible by closed manipulations without residual instability2). However, in extremely rare cases, operative treatment is required for irreducible dislocations caused by incarceration of the plantar plate, interphalangeal sesamoid bone or fracture fragments. To date, about 40 irreducible dislocations of the IP joint of the great toe have been reported1,3,4,5,6,8,10). When force is directed on the joint, intra-articular fractures seem to occur more commonly than ligament ruptures because of the strong collateral ligaments and the stable joint structure7).
In our case, however, the plantar plate and sesamoid bone were found intact while the lateral collateral ligament were ruptured and entrapped into the joint. This is a very rare case that has not been published by any English literature. Shin et al.9) has reported one dislocation of the IP joint of great toe that was irreducible due to entrapped of the lateral collateral ligament into the IP joint. The dislocation occurred while exercising sports called Taekwondo. However, it was an open dislocation in an adolescent, exposing not only the lateral collateral ligament, but also the IP joint associated with the rupture of lateral skin and periosteum. Such an open dislocation associated with an open wound may easily be attributed to the entrapment of the lateral structure. However, it is not easy to presuppose lateral collateral ligament rupture in a case without any open wound. The patient in our study sustained a dislocation due to abnormal varus stress when her entire weight was directed on the joint in an instant moment, which is different from the previously known mechanisms of injury.
When a dislocation of the IP joint of the great toe is not reducible by closed means, the entrapment of the ruptured lateral collateral ligament should be considered as well as the rupture of the plantar plate or sesamoid bone. In particular, when a patient sustained the dislocation on a wooden floor during sports activities using toes, one should suspect the rupture of the lateral collateral ligament. Although we attempted closed methods, the dislocation of the IP joint of the great toe was irreducible. Using the MR images taken preoperatively, we confirmed an entrapped structure. On simple radiographs, the sesamoid bone remained intact, increasing the possibility of the entrapment of the plantar plate alone. But, we confirmed the entrapment of the lateral collateral ligament from MR images and performed operative treatment. If we had had attempted operation based upon the assumption that only the plantar plate was entrapped, both a dorsal incision and a plantar incision might have been possible. Instead, we checked the lesion of the lateral collateral ligament preoperatively using MR images and opted for a dorsolateral incision, making the repair of the lateral collateral ligament easier. Although previous studies have not performed MR images to treat irreducible dislocations of the IP joint of the great toe, we believe preoperative MR images can contribute to the operative treatment of irreducible dislocations by identifying an intraarticular structure that prevents reduction in a case with severe tenderness at the lateral side of the IP joint but whose sesamoid bone appears intact on simple radiograph.



 XML Download
XML Download