

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate the long-term results of treatment of epiphyseal fractures of the distal radius in children.
Materials and Methods
23 cases of distal radial epiphyseal fracture, treated by two methods: group 1, closed reduction (CR) plus cast (6 cases); group 2, CR and K-wire fixation (under anesthesia due to marked translation of the distal fragment and swelling) plus cast (17 cases), were selected for this study. All patients were followed up for more than 1 year (average: 3.2 years). Postoperatively, epiphyseal displacement and epiphyseal angulation were measured on anteroposterior and lateral radiographs. At follow-up, the affected and normal sides were compared. Final results were classified by radiologic (radial inclination, volar tilting and radial shortening) and clinical (limitation of ROM, wrist pain, grip strength and wrist deformity) criteria.
Results
Group 1 had 5 good, 1 fair result; group 2 had 14 good, 2 fair and 1 poor - there was no statistically significant difference between two groups. All cases where the epiphyseal displacement was less than 30% had good results. A poor case showed a radial shortening, wrist deformity and pain due to premature epiphyseal closure. Premature epiphyseal closure was treated by bar resection and free fat, along with corrective osteotomy when necessary and lengthening of radius with or without epiphysiodesis of the ulna.
Figures and Tables
 | Fig. 1Measurement of the epiphyseal angle and displacement of the growth plate of the distal radius on A-P and lateral radiographs.
|
 | Fig. 2(A) A-P and lateral radiographs of an 8-year-old boy who sustained a Salter-Harris type II growth plate injury in the distal radius.
(B) Closed reduction was achieved at the first attempt and a long arm cast was applied. Postoperatively, the epiphyseal angle was 12° and the displacement was 30%.
(C) Radiographs taken 5 years and 5 months after trauma show satisfactory results. This patient showed no clinical complications at the last follow up.
|
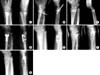 | Fig. 3(A) Radiographs of an 11-year-old boy who sustained a Salter-Harris type II growth plate injury in the distal radius.
(B) Closed reduction was attempted 4 to 5 times and K-wires were used to maintain reduction.
(C) Two years after injury, radiographs show 5 mm of radial shortening and a wrist deformity involving 15° of radial inclination and 15° of volar tilting, due to central bar formation of the distal radial physis. This patient complained of poor grip strength.
(D) Resection of the physeal bar, fat graft and corrective osteotomy of the distal radius were performed (A-P radiographs following surgery).
(E) 2 years and 6 months after surgery, the radius again observed to be 5 mm shorter than the ulna.
(F) Ulnar shortening through the growth plate was performed, with simultaneous epiphysiodesis of the ulna.
(G) Final follow-up radiographs showed a satisfactory result.
|



References
1. Abram LJ, Thompson GH. Deformity after premature closure of the distal radial physis following a torus fracture with a physeal compression injury. Report of a case. J Bone Joint Surg Am. 1987; 69:1450–1453.

2. Aminian A, Schoenecker PL. Premature closure of the distal radial physis after fracture of the distal radial metaphysis. J Pediatr Orthop. 1995; 15:495–498.
3. Arora A, Adedapo AO, Shaw DL. Unusual distal radial epiphyseal injury in a child. Injury. 1999; 30:149–150.
4. Bailey DA, Wedge JH, McCulloch RG, Martin AD, Bernhardson SC. Epidemiology of fractures of the distal end of the radius in children as associated with growth. J Bone Joint Surg Am. 1989; 71:1225–1231.
5. Bragdon RA. Fractures of the distal radial epiphysis. Clin Orthop Relat Res. 1965; 41:59–63.
6. Friberg KS. Remodelling after distal forearm fractures in children. I. The effect of residual angulation on the spatial orientation of the epiphyseal plates. Acta Orthop Scand. 1979; 50:537–546.
7. Gandhi RK, Wilson P, Mason Brown JJ, MacLeod W. Spontaneous correction of deformity following fractures of the forearm in children. Br J Surg. 1962; 50:5–10.
8. Horii E, Tamura Y, Nakamura R, Miura T. Premature closure of the distal radial physis. J Hand Surg Br. 1993; 18:11–16.
9. Kim JR, Pyo SH, Hwang BY. Results of treatment for epiphyseal injuries of the ankle in children. J Korean Soc Fract. 2000; 13:680–685.
10. Kim TS, Park YS, Kim DK, Cho JL. Conservative treatment of moderately displaced S-H type II injury in distal radius -a report of 5 cases-. J Korean Soc Fract. 1997; 10:718–725.
11. Lee BS, Esterhai JL Jr, Das M. Fracture of the distal radial epiphysis. Characteristics and surgical treatment of premature, post-traumatic epiphyseal closure. Clin Orthop Relat Res. 1984; 185:90–96.
12. McLauchlan GJ, Cowan B, Annan IH, Robb JE. Management of completely displaced metaphyseal fractures of the distal radius in children. A prospective, randomized controlled trial. J Bone Joint Surg Br. 2002; 84:413–417.
13. Mizuta T, Benson WM, Foster BK, Paterson DC, Morris LL. Statistical analysis of the incidence of physeal injuries. J Pediatr Orthop. 1987; 7:518–523.
14. Peterson CA, Peterson HA. Analysis of the incidence of injuries ot the epiphyseal growth plate. J Trauma. 1972; 12:275–281.
15. Perterson HA. Partial growth plate arrest and its treatment. J Pediatr Orthop. 1984; 4:246–258.
16. Ray TD, Tessler RH, Dell PC. Traumatic ulnar physeal arrest after distal forearm fractures in children. J Pediatr Orthop. 1996; 16:195–200.
17. Rogers LF. The radiography of epiphyseal injuries. Radiology. 1970; 96:289–299.
18. Salter RB, Harris WR. Injuries involving the epiphyseal plate. J Bone Joint Surg Am. 1963; 45:587–622.
19. Sarmiento A, Pratt GW, Berry NC, Sinclair WF. Colles' fractures. Functional bracing in supination. J Bone Joint Surg Am. 1975; 57:311–317.
20. Schuind FA, Linscheid RL, An KN, Chao EY. A normal data base of posteroanterior roentgenographic measurements of the wrist. J Bone Joint Surg Am. 1992; 74:1418–1429.
21. Tang CW, Kay RM, Skaggs DL. Growth arrest of the distal radius following a metaphyseal fracture: case report and review of the literature. J Pediatr Orthop B. 2002; 11:89–92.
22. Valverde JA, Albiñana J, Certucha JA. Early posttraumatic physeal arrest in distal radius after a compression injury. J Pediatr Orthop B. 1996; 5:57–60.
 XML Download
XML Download