

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Approximately a thousand Korean women die from cervical cancer each year, making it the eighth leading cause of cancer-related death among women (National Cancer Information Center, 2009). Regular uterine cervical cancer screening (UCCS) is recognized as the most effective method for cancer prevention world widely (Waller, Bartoszek, Marlow, & Wardle, 2009). Even though UCCS rates in Korea have dramatically improved since the introduction of nationwide UCCS program in 2001, uptakes among high-risk group aged 40~50 years were still very low, 57.5% (Park & Park, 2010).
Previous studies on UCCS barriers indicated that one important reason women fail to attend UCCS is due to a number of negative feelings such as anxiety, awkwardness, fear, shame, shyness, and embarrassment (Kim, Lee, Lee, & Kim, 2004; Waller et al., 2009). With a valid measure for UCCS embarrassment, embarrassment as an important barrier for gynecological screening can be reliably assessed and women at-risk for cervical cancer can be identified for appropriate uptake or referrals. In addition, a reliable and valid instrument is needed for use in research to determine incidence, prevalence, and risk factors related with embarrassment.
The construct of embarrassment has long been studied as a social anxiety in emotions research. Embarrassment is an unpleasant emotion that people often experience in social interaction and is accompanied by feelings of awkwardness, foolishness and frustration (Edelmann, 1990). Embarrassment often occurs after individuals recognize that they have presented themselves inappropriately and may cause concerns regarding negative social impressions (Ha, 2000). Previous laboratory experimental studies suggest that people often seek to hide expressions of embarrassment. However, embarrassment may nonetheless be evidenced in distinctive patterns of non-verbal and verbal indicators, such as blushing, dampened smiling, gaze aversion, laughing, muscle tension, increased body motion, and speech disturbances (Keltner, 1997).
It is difficult to develop a reliable scale that provides a comprehensive measure of UCCS embarrassment; hence UCCS embarrassment measure is problematic. Several studies suggest that self-reported embarrassment may be somehow different from nonverbal-behaviors because of the function of social inhibition (Costa, Dinsbach, Manstead, & Bitti, 2001) a nd insufficiency of individual's memory (Ha, 2000). Although naturalistic observation might be the best method for evaluating embarrassment, this would be impractical because the state of embarrassment occurs instantly and such an approach would be expensive requiring extensive technical training for data interpretation. In addition, if such studies were to be truly naturalistic, participants would need to be unaware of the measurement, creating ethical issues in the context of intimate examinations.
Most studies have typically used open-ended or semi-structured interviews for the measure of UCCS embarrassment (Park, Chang, & Chung, 2004). These studies have revealed a complex picture in which the degree of UCCS embarrassment is related to several variables. However, there is a lack of clarity on what the term "embarrassment" means. Embarrassment is often synonymously used with shame, shyness, frustration, and discomfort. Meanwhile, descriptive studies of UCCS embarrassment have tended to rely on single-item self-rating scale or binary items (Patton, Bartfield, & McErlean, 2003; Waller et al., 2009). Such measurement may help explain the inconsistent links some studies have documented between embarrassment and UCCS behavior. Waller, et al. (2009) suggests that embarrassment is not strongly predictive of UCCS behavior, despite embarrassment being commonly cited as an important emotional barrier. Similarly, there are discrepancies among reports examining the impact of physician gender on pelvic examination-related embarrassment (Moettus, Sklar, & Tandberg, 1999; Patton et al., 2003). Theses inconsistent findings imply the need for more rigorous UCCS embarrassment measure.
One measure that was specifically developed for the Pap smear related negative emotions provides subscale scores on 12 items of negative cognitive-affective concerns regarding the procedures (Chang & Park, 1999). However, the items did not reflect unique and reactive indicators of physical embarrassment such as blushing and awkward laughing. Another recent measure examines embarrassment in relatively specific domains and incorporates assessment of embarrassment regarding the examination of reproductive organs (Consedine et al., 2007). In this study, women were asked to rate their embarrassment during hypothetical medical examinations in which their sexual/reproductive organs and private parts were exposed, touched, and discussed in front of health care providers. Although promising, the items in this questionnaire do not assess the specific manifestations of reactive bodily embarrassment nor are they specific to gynecological examinations.
The uterine cervical cancer screening questionnaire (UCCSEQ) was originally developed for the purpose of measuring the distinctive aspects of UCCS embarrassment (Cho, 2003). The UCCSEQ has the four-factor structure that has been grounded in the conceptualization of embarrassment (Cho & Chung, 2002-a). That is, UCCS embarrassment is viewed within the dramaturgical interaction or self-presentational model of embarrassment (Goffman, 1959, 1967; Leary & Kowalsaki, 1995). In this model, embarrassment is a multidimensional construct that involves a variety of unique and easily noticeable reactions resulted from a fear of losing face in social interaction. UCCS embarrassment is thus viewed as consisting of cognitive-emotional, physiological, verbal and non-verbal behavioral responses which occur to cope with a fear of negative social impression regarding UCCS. While the UCCSEQ was preliminary validated in the empirical study (Cho, 2003) to examine the effect of the desexualization care guided by dramaturgical interaction on women's embarrassment during UCCS, its psychometric attributes have not yet been reported.
The UCCSEQ is merely a psychometric measure and does not directly assess UCCS embarrassment. Thus, the underlying assumption tested was that the UCCS embarrassment being measured and the items included in the scale form one-dimensional construct. In this study, the construct of UCCS embarrassment was assessed by Rasch model, which has been known to be as a complementary method to the classical test theory (CTT). The critical problem with the classical test theory (CTT) is that it implies that one can directly infer, e.g., UCCS embarrassment by summing responses and calculating a total score, assuming that all items are supposed to be of identical importance. However, in reality some items are more important to person than other items. A UCCS woman's strong agreement with an item like "I find that I become a stammer" indicates that a great problem than does a strong with an item like "I find that I tend to close my eyes". Thus, it seems to suggest that the data items representing different level of importance to the UCCS embarrassment should not be analysed so that the total score reflects this value of "importance" of the item's contribution to the total scale value. Rasch model has a merit for constructing a line of measurement with the items ordered hierarchically on this line according to their importance data (Bond & Fox, 2001). Thus, the validity of measure can be assessed by examining whether all items work together to measure one-dimensional construct. Considering the fact that the UCCSEQ has been the only self-administered measure readily available in this specific area, the current study was carried out to evaluate psychometric properties of the UCCSEQ with complementary use of Rasch model.
METHODS
A. Participants
Participants were eligible for the validation study if they were aged above 20 years, not pregnant, had not received an abnormal UCCS result in the last 6 months and had not a hysterectomy. The sample was recruited from four clinical sites: one gynecologic clinic and health screening center at one university hospital and two other out-patients based gynecologic clinics, in Gyeongju. The reason for the selection of sampling site was to collect the data of public and private UCCS. A total of 380 women were eligible to participate in this study and 339 (82.9%) women gave informed consent. Of these, 16 failed to complete the survey adequately and, as a result, the data from 323 women providing complete data was included in the final analysis.
B. Pilot study
In July 2008, the UCCSEQ was administered to 9 women who had a UCCS at a university health screening center and gynecological clinics. It took 10~15 min for them to complete the questionnaire. All women found the 29 items to be clear and easy to understand, and none had difficulty with the response categories.
C. Procedures
Eligible women were invited to the questionnaire with assurance that there would be no disadvantages regarding the UCCS in case they declined to participate whenever they feel uncomfortable. After signing a written informed consent form, women completed a self-rating open-ended and closed questionnaire to assess demographic variables. Immediately after her UCCS, the participants were invited by research assistant into a separated place and left alone to complete the UCCSEQ and related psychometric measures. Participants were given a gift voucher valued of US$5 for completion of the survey. Data were collected during the period from August to September 2008.
D. Measures
All consenting participants completed a questionnaire package measuring UCCS embarrassment, general medical embarrassment, dispositional embarrassability, and Pap smear related negative emotion. A demographic questionnaire elicited information regarding self-reported age, education, household income, marital status and employment. Given the nature of UCCS experience, women's gynecological characteristics including reports of prior UCCS was also recorded.
a. Uterine cervical cancer screening embarrassment questionnaire (UCCSEQ)
The UCCSEQ is a 29-item self-report questionnaire and consists of four domains; verbal, behavioral, physiological and cognitive-affective perceptions (Cho, 2003). The UCCSEQ verbal-subscale was comprised of 4-item verbal cues such as being a stammer. And, non-verbal behavioral-subscale was consisted with 13-item non-verbal disturbances such as avoiding eye contact. Then, the physiological-subscale was composed with 3-item involuntary physiological responses such as blushing. Finally, the cognitive-affective subscale included 9-item self-awareness of unwanted social impression such as feelings of shyness or shamed. Each item is rated using 7-point Likert scales, ranging from 1, 'not at all' to 7, 'a very great deal', with lower scores indicating feel less embarrassed.
b. Visual analogue scale of UCCS embarrassment
The participants were asked to make ratings of pre, during, and post-Pap smear embarrassment on the 100 mm VAS for convergent validity; all ratings were made immediately after the screening. In the previous study, single-item scales have been used to rate the extent of embarrassment during pelvic examination (Cho & Chung, 2002-b; Patton et al., 2003).
c. Medical embarrassment questionnaire
Two subscales from the Medical Embarrassment Questionnaire (MEQ) were used to determine convergent and discriminant validity (Consedine et al., 2007). This modified 31-items general medical embarrassment scale use 5-point Likert scale ranging from not at all to very much and generates two components identified as 'bodily embarrassment' and 'judgment concern.' This scale has been found to have good internal reliability with a α values .96 for the bodily subscale and .90 for the judgement subscale (Consedine et al., 2010). The reliabilities in the current sample were .93 for the bodily subscale and .83 for the judgment subscale.
d. Susceptibility to Embarrassment Scale
The Susceptibility to Embarrassment Scale (SES) is a 25-item self report scale measuring broader dispositional embarrassability characteristics (Kelly & Jones, 1997). Participants were asked to rate each of the 25 items on a 7-point Likert scale, ranging from not at all true to exactly true, to test whether UCCS embarrassment was distinct from dispositional embarrassment. This scale has been shown to have good internal reliability with a α values between .84 (Cho & Chung, 2002-b) and .90 (Kelly & Jones, 1997). The α in the present sample was .93.
e. Pap smear related Negative Emotion
An original 12-item Pap smear related negative emotion scale (Chang & Park, 1999) was administered to all participants for convergent validation. Participants respond to each items on a 5-point Likert scale ranging from not at all true to exactly true. This scale has been found to have good internal reliability (α=.86). The α in the present sample was .98.
E. Ethics
The study was approved by the Dongguk University Gyeongju Hospital Institutional Review Board (DUGH 10-30). Women who met the criteria of this study were introduced by doctors or nurses to a research assistant, who explained the purpose of the study, the nature of participation, the ethical considerations of confidentiality and anonymity, as well as their voluntary nature of any involvement.
F. Data analysis
In the current analysis, Rasch model was applied to preliminary 29 items (Cho, 2003); (a) to improve the item-pool quality by calibrating item difficulty, Infit and Outfit Mean Square (MnSq), and point-measure correlation which enables detecting an inappropriate item that should be deleted, or replaced; (b) to examine the 7-point category functioning by calculating frequency of category use, observed person measure, threshold measure and outfit Mnsq for each category which estimate the rating scale structure and its utility (Bond & Fox, 2001). "Item difficulty" for the 29 items was estimated and each respondent's scores in logit unit were identified. In order to determine how well each item contribute to global embarrassment measurement, χ2 fit statistics, known as "Infit" and "Outfit" MnSq were calculated. Item MnSq values≤1.2 are ideal (Linacre & Wright, 1991; Linacre, 2002). In this study, the predetermined fit criteria for item removal were Infit MnSq≤1.5 and Outfit MnSq≤2.0 (Ko et al., 2008). "Point-measure correlation" (equivalent to classical item-total correlation) was used to examine the discriminative power of each item (Linacre & Wright, 1991). The frequency of category use indicates how many persons have been rated in that particular category, estimating the relative locations of the person and items, 'targeting'. "Observed person measures" was examined to confirm whether response category 3 is expected to be higher than for category 2. "Threshold measure" is expected to increase with increasing category number. An "outfit MnSq" for each category was estimated to examine the consistency of use of the category.
Exploratory factor analysis on the 29 items was used to examine the potential sub-dimension of the UCCSEQ construct. Cronbach's α coefficients were calculated to establish internal reliability in the sub-scales and in the total 29-item scale. To assess the relative independence of the sub-scales, the Pearson correlation coefficients were calculated. Convergent and divergent validity was established by examining the correlations between the UCCSEQ, 100 mm VAS ratings, the MEQ, the SES, and the measure of Pap smear related negative emotions to determine. Known group validity was examined by comparing the CCCES scores of women who were high in SES score vs. those who had low score of SES. All statistical analyses were conducted using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) and WINSTEPS Rasch Analysis computer program +8.0.
RESULTS
A. Characteristics of the respondents
Overall, the mean age of the sample (n=323) was 42.7 (SD=8.38), ranged 26~64 years. The majority of the respondents (86%) had a high school education or higher, only 8% were not married, and 52% had full-time jobs. 43.4% reported household's monthly income over 3.0 million won ($3,200). The majority had, on average, been pregnant 2.7 times (SD=1.41) and majority (81.7%) had at least two children. Most participants (70.6%) had no history of gynecological disease. More than half of the participants (53%) had their first UCCS during their thirties and the mean frequency of UCCS women reported in the preceding 3 years was 1.98 (SD=0.82), a frequency range of 1-3.
B. The psychometric structure and reliability of the UCCSEQ
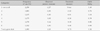
The item difficulty of the 29 items ranged from -.50 to .59 logits (Mean=0, SD=0.31) for the most difficult and least difficult items respectively. The person ability of the items ranged from -3.90 to 3.50 logits (Mean=-.43, SD=1.28). As shown in Table 1, all the 29 items adhered to acceptable fitting criteria for item inclusion (infit and outfit MnSq≤1.5 and 2.0, respectively) in range 1.83~.78, verifying as the unidimensional construct. The item-total correlations of the 29 items are adequate (all value≥0.30).
Across all the 29 items the frequency distribution of 7 category use was not skewed towards the lowest or highest categories, indicating good targeting. Summary statistics for the 7 rating-scale categories use are shown in Table 2. The "Frequency of Use" of all categories was high, indicating that no category was underused and also that there were sufficient observations of each category for a stable measurement. The frequency of category use from 1 to 7 was fairly even. Category 1 - 'not at all' agree to the statements of UCCSEQ items was used approximately 3 times more often than any of the other 6 categories (count=2258). This implied that the majority of subjects were hardly embarrassed on many statements of UCCSEQ items, supporting the result that the mean person ability (-.43) was lower than the mean item difficulty (0). The "observed person measures" increased from a low category representing low embarrassment to a high category, demonstrating no need for collapsing on rating categories. The "threshold measures" increased with the rating category value, indicating that the raters are most likely to choose from 1 up to 7 as their embarrassment increases. The total range of the 7 category thresholds was 1.75 logits, suggesting that the rating function could be improved with the category number lesser than 7. The "outfit MnSq" for all categories was ≤ 1.50, indicating no extreme misuse in any of the categories.
Principal Components Factor Analysis with Varimax rotation on the preliminary 29 items was carried out to determine the construct of UCCS embarrassment. Although the fit of the hypothesized four-factor model analysis was moderately high accounting for 73.7% of the total variance, there were several items misfitting to the underlying conceptual model with loadings ≤ .40. Inspection of the scree plot suggested that a three-factor solution (70.2% variance explained) was more readily interpretable. Consequently, a preliminary solution of three correlated factors were selected as the best fit to the data base d on eigen values ≥1 in which all communalities were above .30 and all items loaded at least .40 on only one factor. In a subsequent three-factor model analysis process, it was revealed that all items describing emotional-cognitive aspects of embarrassment loaded on only one factor, while items on verbal disturbances, behavioral predicaments and physiological responses tended to be double-loaded. Having considered that these three attributes can be broadly conceptualized as bodily embarrassment, two-factor model analysis was ultimately conducted, resulting in 66.2% of the total variance. Having deletion of four items (I feel like running away, firmly grabbed my hands, I winced my body, and my body is getting rigid and tense), all items related distinctly into one of the two factors with correlation coefficients≥.5. For the purpose of psychometric testing, these four items were dropped from the instrument because these items did not load properly on any factors, due to by either the factor-loading≤.40 or a low rotated factor score≤.1. Therefore, two factors containing 25 items were retained for further structural model fitting. The final 25 items loaded on two factors explained 67.3% of the total variance (Table 3). These two factors were labeled according to their contents as well as prior conceptual frameworks: "bodily embarrassment" displaying a various range of verbal disturbances, behavioral predicament and physiological impediment" (F1: 17 items) and "apprehension of unwanted or unintended social face" (F2: 8 items) and accounted for 36.0% and 31.3%, respectively (Table 3).
As shown in Table 4, both subscales (F1, F2) and total the UCCSEQ Cronbach's α demonstrated adequate reliability (Cronbach's α=.96, .97, .97, respectively).
C. The evidence of construct validity
Subscale-to-subscale and subscale-to-Overall UCCSEQ correlations were in the expected direction and of general magnitude (F1-F2: r=.71, p<.001; F1 & Overall UCCSEQ: r=.96, p<.001 and F2 & Overall UCCSEQ: r=.87, p<.001), indicating that the UCCSEQ had good construct validity.
Table 4 shows that the scores of both the two UCCSEQ subscales and overall UCCSEQ were positively associated with other closely related convergent validation measure-the 100 mm VAS of embarrassment, the two subscales of MEQ, the SES, and Pap smear related negative emotion. As would be expected (see Consedine et al., 2011), the UCCSEQ subscales (F1: z=4.95, p<.001; F2: z=2.68, p<.05) and overall UCCSEQ (z=3.89, p<.001) were more closely correlated with the MEQ's bodily embarrassment factor than with the judgment concern score. These findings provide good evidence of the discriminant validity of the subscale scores.
It was hypothesized that women showing high dispositional embarrassability, in comparison to those with a low score, would feel more embarrassment during UCCS. As expected (Table 5), women reporting higher trait embarrassability (with mean score ≥ 79 on SES) scored higher than those with lower trait embarrassability (with mean score <79 on SES), indicating that the UCCSEQ had good known-group validity.
DISCUSSION
The purpose of this study was to describe both the psychometric properties of self-administered UCCSEQ and the function of 7-point rating categories. The preliminary items pool was found to be a unidimensional set for UCCSE measurement and successfully functioned with the 7-point rating categories. As hypothesized, UCCS embarrassment was multi-componential and could be explained by two distinctive, reliable, and valid properties-one circumscribing bodily embarrassment across a range of behavioral and physiological impediment and the other representing women's apprehension of unwanted public face.
A. UCCS: What are women embarrassed about?
As previous studies suggest that women may be embarrassed by either bodily predicaments (or exposures) (Keltner, 1997) or the apprehension of an unintended public-face (Ha, 2000), the 25-item UCCSEQ can also be constructed into two sub-domains. Bodily UCCS embarrassment can be assessed by verbal, non-verbal, and physiological indicators of embarrassment. For example, women tended to report verbal difficulties such as'voice trembled', 'voice is altered', 'become a stammered', 'become speechless', and 'awkward laughing'. In addition, women who were embarrassed reported a number of behavioral embarrassment manifestations such as'grip the sidebar of the examination bed tightly', 'bottoms keep moving upward from the examination table', 'keep touching face with hands', 'thighs get turned inward with a full strength', 'clench teeth', 'keep trying to pull skirt downward', 'tend to close eyes', and'tend to avoid eye contact'. Women also reported a number of reactive physiological changes such as'heart keeps beating', 'face gets blushed', and 'get thirsty'. Meanwhile, UCCS embarrassment by the apprehension of an unintended public-face can be manifested through aversive emotions such as, shyness, self-consciousness, and feeling uncomfortable, awkward, ashamed or uneasy arising prior to the screening.
B. UCCS embarrassment: Evidence of validity and reliability
In current study, the 29 items which were originally developed as the preliminary UCCSEQ in the previous study (Cho, 2003) was found to be as a valid measure within Rasch model. Meanwhile, given that the preliminary UCCSEQ was composed of four-domain; verbal, non-verbal, physiological and cognitive-affective embarrassment, it seems reasonable to assume that the 29 items (Cronbach's α=.96) were readily reduced into the 25-items (Cronbach's α=.97) under two distinct dimensions.
As expected, the two factors of the UCCSEQ were related to one another and showed a pattern of relations with other measures indicating convergent as well as discriminant validity. Our expectation, that the two factors of the UCCSEQ would be positively associated with the 100 mmVAS, general medical embarrassment, Pap smear related negative emotion and, to lesser degrees, dispositional embarrassment was confirmed (Table 4), with associations being stronger for conceptually more similar constructs. For example, correlations with other related measures of embarrassment ranged from .57 to .61, while those with dispositional embarrassment were between .36 and .32. These comparatively weak associations between the UCCSEQ and dispositional embarrassment suggests that although the UCCSEQ two factors are related to dispositional embarrassment, they are distinct from the dispositional measure and appear to capture the response to specific elicitors in the UCCS context.
Other findings provided evidence that the two factors of the UCCSEQ are separable and capable of assessing slightly distinct aspects of the general construct. First, dispositional embarrassment was more strongly correlated with 'bodily predicament' factor than to the 'apprehension of undesirable social face' factor (Table 4). In addition, the analysis of known-group validly showed that both bodily embarrassment and apprehensive embarrassment for those high in trait embarrassment were greater than those low in trait embarrassment (Table 5). It may be that bodily embarrassment in UCCS are more closely linked to dispositional response patterns and less contextually sensitive than embarrassments caused by the apprehension of unintended public face. On the other hand, items from the apprehension of unintended public face are closely linked to the interactional situations between health care provider and women during procedures. Above all, this study suggests that the bodily predicament factor should be more directly to UCCS behavior, perhaps particularly so among women high in trait embarrassment.
C. Implications, limitations, and direction for future study
Rating scale analysis in this study showed that no collapse or addition of rating is necessary in CCES. However, given that the respondents tend to response to relatively easy rating categories and the total range of 7-category thresholds was smaller than expected, the category number might be reduced to something lesser than 7 in future study.
Having considered a careful and objective assessment of specific domains of embarrassment can guide systematic interventions to address possible sources of non-attendance in UCCS, the current study provides some preliminary guidance - it is the bodily predicament that seems to prevent screening attendance. Therefore, the specific bodily predicaments should be given special consideration as possible deterrents to UCCS non-attendance. Further work might continue this differentiation in other types of cancer screening such as breast self-examination or colorectal cancer screening (Consedine et al., 2011). In addition, given the strong preference of same-gender health personnel for intimate health care such as gynecological care (Lodge et al., 1997) or colorectal screening (Consedine, Reddig, Ladwig, & Broadbent, 2011), the subscale of bodily predicaments could be applied to address an unmet need for intimate bodily care in which embarrassing care is delivered by the opposite-gender health care provider.
It is assumed that bodily embarrassment, especially for those high in trait embarrassment, more likely to deter UCCS attendance, thus interventions for enhancing dramaturgical bodily skills regarding the UCCS-procedures (Cho, 2003; Henslin & Biggs, 1971) should be targeted at this risk-group. Even though we have concentrated on bodily embarrassment, it seems likely that discrepancies in the social image projected between health personnel and women screened, such as apprehension of immodest or stigmatization could deter screening attendance (Waller et al., 2009). Therefore, public consensus should be progressively established by mass media campaigns focusing on UCCS attendance as being a normative social behavior.
Although the above contributions presented, the results of the study should be interpreted with caution due to a number of potential limitations. Given that we used a self-rating questionnaire retrospectively in a cross-sectional design, the components of the UCCSEQ would not be guarantee for a real time self-reporting data or distinctive physiological and behavioral responses reported on other studies (Leary & Kowalsaki, 1995).
Another limitation of this study may be a lack of representativeness of the samples. The feeling of 'embarrassment' as a mechanism of self-control might reflect the extent of the civilization of the society (Edelmann, 1990). Women, therefore, belonging to an urban society may perceive the UCCS embarrassment differently from the current rural samples. The fact that the views of women screened by female doctors and were not or never screened in preceding three years were not reflected should also be considered. Given that the UCCS embarrassment seems to have universal/common attributes (Henslin & Biggs, 1971) while related factors could be varied (Edelmann, 1990), a psychometric validation study with a larger and more diverse sample in different cultural settings is needed.
Furthermore, the UCCSEQ merely measures the degree of cognitive-affective and bodily reaction which women instantly feel or react in embarrassing moments. Therefore, it is necessary to expand the instrument to cover comprehensively other related factors, such as antecedents or consequences, which were not specifically described in UCCSEQ items.
CONCLUSION
The UCCSEQ may be used to evaluate the degree of embarrassment in other health services such as pelvic examination, colonoscopy, breast self-examination, urinary incontinence consult, and safe sex education. In many examinations, clients are required to expose their private body or consent to intimate interactions with medical personnel, resulting in the avoidance of health-promoting behaviors. We also hope that the UCCSEQ will be used for the development of a theoretical model for embarrassment-prevention practice, since critical pathways in nursing assessment, implementation and outcome of embarrassment remain poorly understood.




 XML Download
XML Download