

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is one of the most common malignancies worldwide [1] and the second most common cancer among Korean women [2]. Although the incidence rate for breast cancer is increasing, the survival rate is also increasing owing to advances in diagnosis and treatment techniques compared to those of the past [345]. In addition, as cancer survival rates and average life expectancy have increased, the incidence rate of multiple primary cancers (MPCs) in addition to breast cancer has also increased [6]. As a result, interest in MPCs has increased, and various studies have been performed.
The criteria for diagnosing MPCs are (1) definite malignant features of each mass; (2) each mass should be separated from other masses; and (3) the possibility of metastasis should be excluded [7]. In addition, the time interval between MPC occurrences is usually defined as synchronous if it is less than 6 months and metachronous if it is more than 6 months; however, there is no definite period. Several studies have shown that the prognosis for metachronous MPCs is better than that for synchronous MPCs [8910].
Although many studies have been performed regarding MPCs, these have usually taken the form of case reports [111213]. There have been several analytic clinical studies on MPCs, but few analytic clinical studies related to breast cancer with MPCs have been reported. Additionally, there have been very few large-scale studies of MPCs. Therefore, this study was designed to compare the characteristics and prognosis of patients with breast cancer alone with those of patients with breast cancer and MPCs using large-scale data.
METHODS
Data collection
In this study, we used data approved by the Korean Breast Cancer Society registration system (KBCR). Since 1996, the KBCR has been registering cases submitted by breast surgeons at 110 training hospitals nationwide [21415]. The cause and date of death in the data were used in connection with the Korea Central Cancer Registration Data of the Ministry of Health and Welfare in collaboration with the Korean National Statistical Office to compile complete death statistics which were updated through 2014. This study was approved by Daejeon St. Mary's Hospital Institutional Review Board (No. DC17RESI0063).
Patients and clinical factors
Of the 161,716 patients who underwent surgery for breast cancer, 41,841 patients were included in this study after the exclusion of patients younger than 18 years or of unknown age, and patients with observation period errors or missing data for analyzed clinical factors (Figure 1). Pathologic stage was determined based on the postoperative pathologic stage; however, for the 2,759 patients who underwent neoadjuvant chemotherapy or palliative chemotherapy, the preoperative clinical stage was used. The clinical characteristics analyzed were age, family history, breast cancer TNM stage, estrogen receptor (ER) or progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), Ki-67, p53, and MPCs. The range of family history was limited to breast cancer. The criteria for classifying age and Ki-67 into two groups, respectively, were set near the respective mean values. Overall survival was calculated from the date of surgery for the breast cancer to the date of death from any cause as specified in the data. Survival rates were compared based on overall survival. The extent of MPCs was based on the data specified, but excluded breast cancer in the MPCs category. The time interval between breast cancer and MPC occurrence was measured in units of years, and when two or more MPCs were present in one patient, the shorter time interval between occurrences was adopted.

Statistical analysis
The data were compared with clinical characteristics according to the presence or absence of MPCs using Student t-tests and chi-square tests. We analyzed the factors associated with MPCs using binomial logistic regression and analyzed the overall survival differences according to presence or absence of MPCs using the Kaplan-Meier method and Cox proportional hazards model. We performed subgroup analysis of MPCs with regard to whether they affected survival, such as the number of MPCs excluding breast cancer, the order of occurrence of breast cancer and MPCs, the time interval between breast cancer and MPC occurrence, and sites of occurrence of MPCs. Statistics were analyzed using SAS version 9.3 (SAS Institute Inc., Cary, USA) and SPSS version 22.0 (IBM Corp., Armonk, USA), and p<0.05 was considered to be statistically significant.
RESULTS
Characteristics of multiple primary cancer
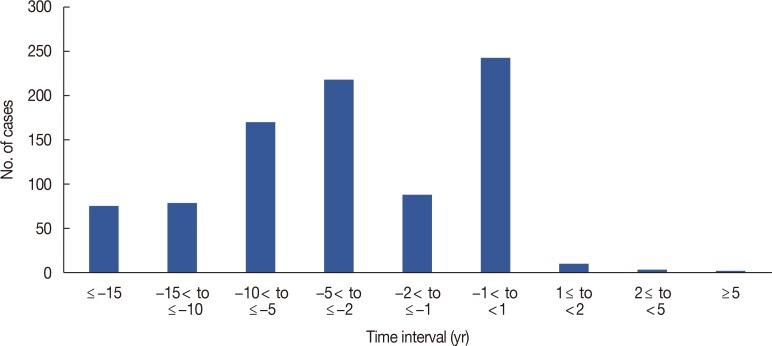
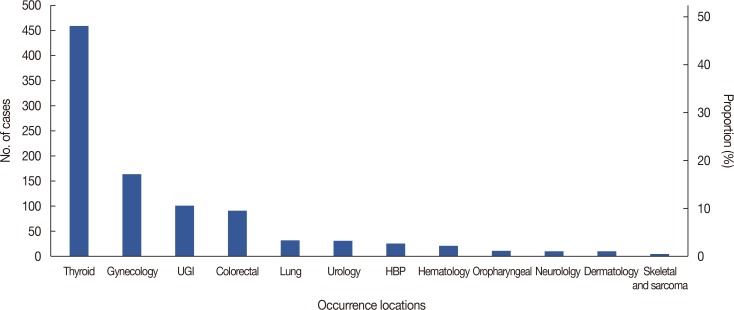
The median follow-up period was 39 months (range, 0–289 months) for the 41,841 patients who underwent surgery for breast cancer from November 1990 to December 2014. A total of 950 MPCs were observed in 913 patients, and 37 patients were found to have two or more MPCs. For the observed MPCs, the occurrence site, the time interval relative to the occurrence of breast cancer, and the order of occurrence in relation to breast cancer are presented (Supplementary Table 1, available online). The first incidence rate for MPCs was higher than for breast cancer (Figure 2). Thyroid cancer was the most common MPC (n=461, 48.5%), followed by gynecologic cancer (n=165, 17.4%) (Figure 3).
Clinical characteristics
The clinical characteristics of the enrolled patients were compared according to the presence or absence of MPCs. The presence of MPCs was significantly higher than the absence of MPCs in patients with the following characteristics: mean age (54.29±11.33 years), age 50 years or more (61.2%), positive family history (12.5%), Tis-1 (65.8%), N0 (69.2%), stage 0–I (55.5%), and HER2 positive (27.8%) (Table 1).
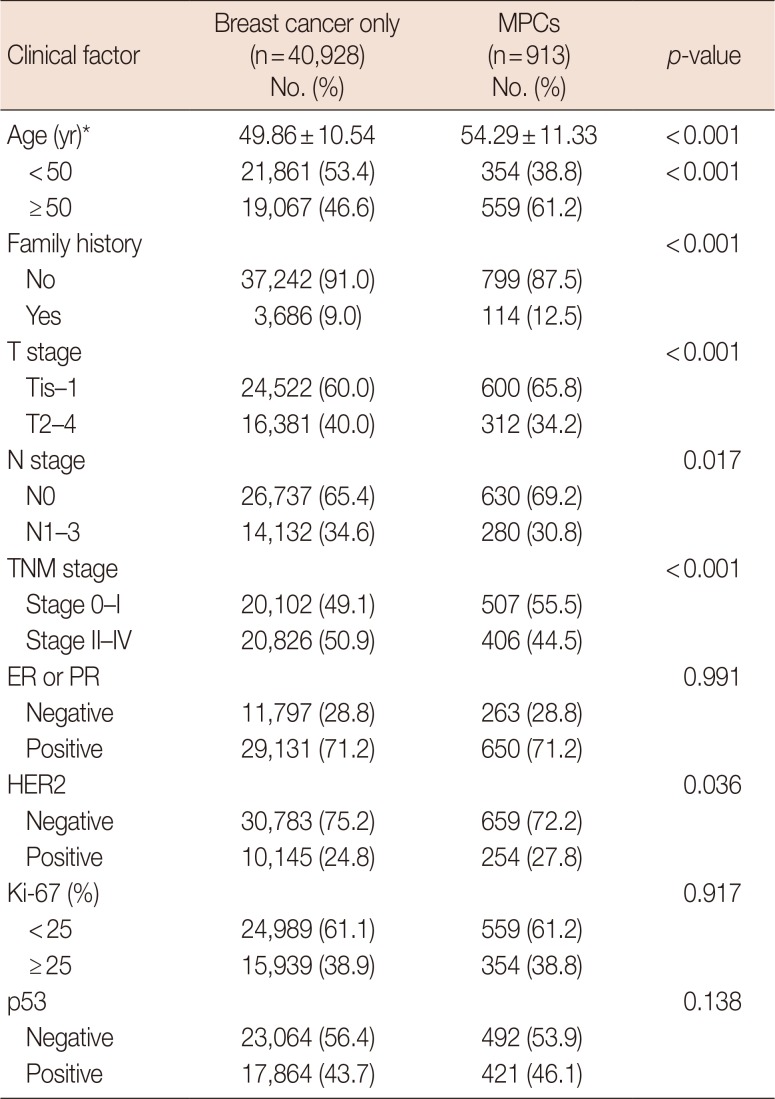
Table 1
Clinical characteristics of breast cancer with or without MPCs
![]()
Factors associated with multiple primary cancer
Factors significantly associated with MPCs were age 50 years or more, positive family history, stage 0–I, and HER2 positive in univariate analysis, and age 50 years or more, positive family history, and stage 0–I in multivariate analysis (Table 2).
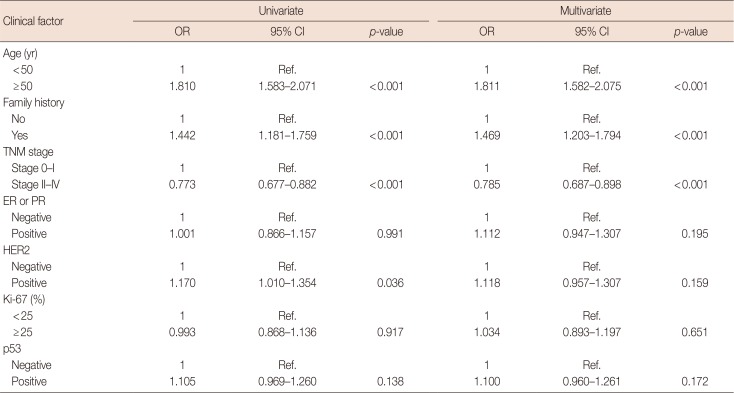
Table 2
Univariate and multivariate analysis for clinical factors associated with MPCs
![]()
Survival analysis
The 5-year survival rates were 93.6% and 86.7% and the 10-year survival rates were 87.5% and 70.4% (log-rank p<0.001) in patients with breast cancer only or with MPCs, respectively (Figure 4). Following adjustment for other factors, the hazard ratio (HR) for overall survival increased with MPCs (HR, 2.192; p<0.001). Other independent factors affecting overall survival were age, pathologic stage, ER or PR, Ki-67, and p53 (Table 3).
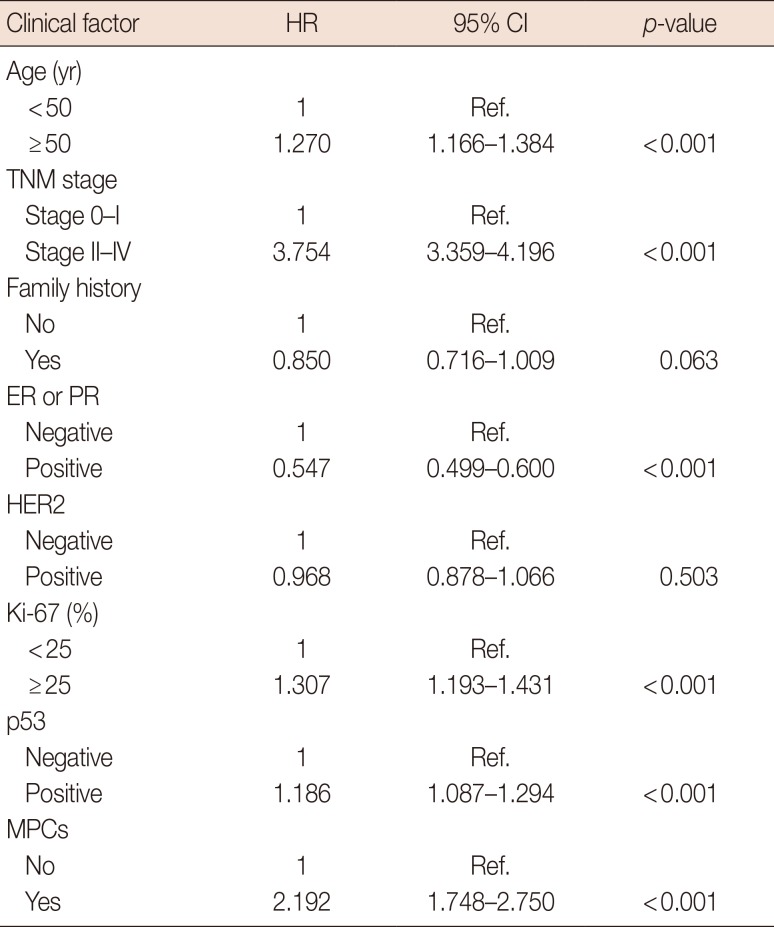
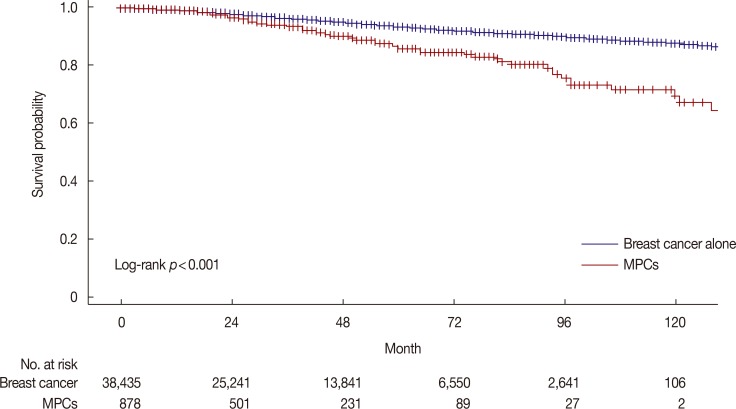
Table 3
Clinical factors affecting overall survival
![]()
Survival differences between the factors related to multiple primary cancer
We compared the survival rates of 913 patients with breast cancer with MPCs based on factors related to MPCs and found that the survival rate of patients with two or more MPCs was worse than that of those with a single MPC (HR, 2.853; p=0.029). There was no significant survival difference between breast cancer and MPCs among the 630 patients who had a time interval of more than 1 year between breast cancer and MPC occurrence, whichever occurred first (HR, 0.876; p=0.832). Additionally, analysis of patients with time intervals between breast cancer and MPC occurrence of 5 years or more and less than 10 years (HR, 0.432; p=0.023) or 10 years or more (HR, 0.379; p=0.010) showed better prognosis in these groups than in patients with a time interval between occurrences of within 1 year. Thus, longer time intervals between occurrences resulted in better prognoses (Table 4).
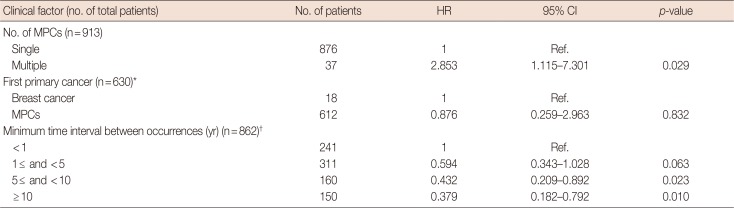
Table 4
Subgroup analysis of clinical factors affecting overall survivals of MPCs
![]()
Relationship between multiple primary cancer and survival at each breast cancer stage
Breast cancer TNM stage, like the presence of MPCs, was also a factor that affected survival in the present study. Adjustment and analysis of other factors to determine whether MPCs affected prognosis at each stage revealed that the HR of overall survival was relatively lower when the breast cancer stage was higher; the exception to this was stage IV (Table 5).
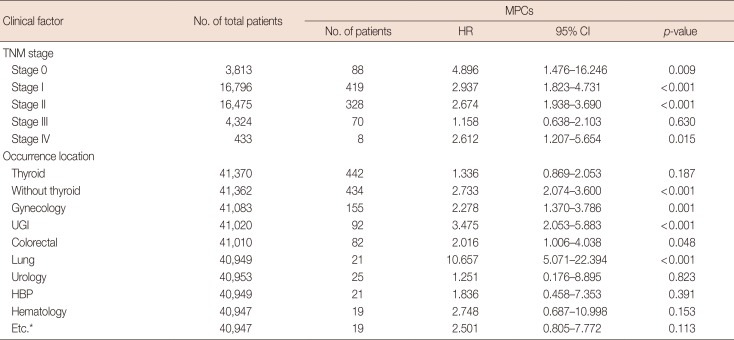
Table 5
Clinical factors affecting overall survival of MPCs for whether TNM stages and occurrence locations of MPCs
![]()
Relationship and survival for site of multiple primary cancer
When we compared survival rates according to the MPCs in each site of occurrence of MPCs, the MPCs affecting the prognosis of breast cancer were gynecologic cancer, colorectal cancer, upper gastrointestinal cancer, and lung cancer. Of these, lung cancer had the greatest effect on survival (HR, 10.657; p<0.001). MPCs excluding thyroid cancer also affected the prognosis. Thyroid cancer was the most common primary cancer, but was not related to breast cancer prognosis (Table 5).
DISCUSSION
Breast cancer is one of the most common cancers worldwide, but breakthroughs in diagnostic and therapeutic technologies have improved survival. According to some studies, as cancer survival rates have increased, the incidence of MPCs has also gradually increased; this phenomenon appears to be due to a combination of genetic backgrounds and environmental effects [161718]. In the present study, as MPCs were detected prior to the diagnosis of breast cancer, it is thought that the survival of other cancers has improved, and breast cancer incidence has increased, leading to an increase in MPCs.
The mean age of the MPC group was higher than that of the breast cancer only group in this study. Age was associated with MPCs and affected the prognosis. It has been reported in other studies that the incidence of MPCs increases with age [9192021]. Increasing age is thought to increase the incidence of MPCs owing to the increased cumulative exposure to various environmental factors and increased risk of genetic mutations. Family history was also associated with MPCs in the present study. Yoshimoto et al. [22] reported that family history is one of the factors that increases the incidence of MPCs. In this study, only a family history of breast cancer was analyzed, but some genetic risk factors for breast cancer appeared to affect the development of MPCs.
p53 is a tumor suppressor protein and is also associated with certain genetic disorders. p53 mutation plays an important role in various cancers. The most common genetic disease of TP53 mutation is Li-Fraumeni syndrome, which is characterized by a relatively high incidence of multiple cancers. Park et al. [23] evaluated 14 patients with Li-Fraumeni syndrome and found that six out of 11 women had breast cancer, and five of them had breast cancer and MPCs. Similarly, Mai et al. [24] reported that among women with Li-Fraumeni syndrome, breast cancer occurs most frequently in women with germline TP53 mutations. In the present study, we did not establish any association with MPCs, but p53 was associated with breast cancer prognosis. In a study of p53 status in patients with MPCs, Kikuchi et al. [25] showed that p53 overexpression could be a prognostic factor for breast cancer.
The number of patients with MPCs after breast cancer in the present dataset was not large enough to allow analysis of the treatment of breast cancer. Several other studies have shown that treatment of primary cancers may be a risk factor for MPCs. Berrington de Gonzalez et al. [26] reported that radiation therapy increases the risk of MPCs. Thyroid cancer accounted for the largest proportion of the MPCs in this study, and radioactive iodine was administered in some cases; this treatment may have led to an increased incidence of breast cancer, as observed in several other studies [2728]. In the present study, however, as the rate of radioactive iodine therapy could not be identified in Korea, these relationships were not elucidated. Rather, it is thought that the high incidence of thyroid cancer alone is the main reason. MPCs may occur after treatment for Hodgkin's lymphoma, with breast cancer the most common MPC, a finding thought to be the result of radiation therapy to the chest [1829].
In the present study, patients with breast cancer with MPCs had worse prognoses than those with breast cancer only. Lee et al. [20] reported similar results in that patients with MPCs had a worse prognosis than those with breast cancer only in a single institution study. We defined the time interval between breast cancer and MPC occurrence as within 1 year when breast cancer and MPCs were diagnosed in the same year. Correspondingly, the prognosis was significantly worse when the time interval between breast cancer and MPC occurrence was short. It is thought that a double primary cancer shows a synergistic effect similar to distant metastasis of a single primary cancer when developed over a short period of time. Eliyatkin et al. [8] reported that in 45 patients with bilateral breast cancers, patients with synchronous breast cancer had significantly worse prognoses than patients with metachronous cancer. Shan et al. [9] reported that in 283 patients with MPCs from among 27,642 patients with lung cancer, similar results to those of the above study were obtained. The present study was more illuminating as the time interval between occurrences was further subdivided, and the longer the time interval between occurrences, the better the prognosis.
With respect to breast cancer TNM stage, lower stage breast cancer was associated with MPCs. Most breast cancer cases with MPCs in our data were secondary primary cancers. If cancer is present prior to the occurrence of breast cancer, it is thought that more frequent screening leads to greater early detection of breast cancers. In patients with breast cancer and MPCs, the higher the stage of breast cancer, the lower the survival rate; however, early breast cancer had an increased prognostic impact on MPCs. Lee et al. [20] compared survival by stage-matched analysis and reported a difference according to MPCs at the lower stages. It is thought that the survival rate of breast cancer is high at lower stages, and the influence of MPCs on the survival rate is increased.
In the present study, prognosis by MPC site of occurrence differed according to the MPC. Particularly in the case of thyroid cancer, which has a relatively good prognosis, the prognosis of breast cancer was not affected despite thyroid cancer showing the largest number of cases. Zhang et al. [30] reported that the development of thyroid cancer after breast cancer results in a worse prognosis than that of breast cancer alone; however, this finding may have been the result of differences in the analyzed groups. There were no significant differences in prognosis among hepato-biliary-pancreatic cancer, urologic cancer, hematologic cancer, and the other small number of cancers, a result that may be due to the small number of patients or deaths. Therefore, further analysis will be required to confirm this finding.
This study employed a more objective assessment of the differences in breast cancer prognosis according to MPCs using large-scale data. However, there were several limitations to the study, including its retrospective design. Additionally, the data were limited to the year of occurrence to confirm the order of occurrence when the time interval between occurrences was less than 1 year. Although we used large scale data, such data were passively obtained from medical records at multiple medical institutions, leading to missing data such as secondary MPCs after surgery for breast cancers. Even after cancer registration, it is considered necessary to update patient information on a regular basis. The number of patients with MPC and breast cancer TNM stage IV was very small, so we were limited in our ability to explain the influence of type of cancer on survival rates.
In conclusion, MPCs were a poor prognostic factor for patients with breast cancer. Two or more MPCs and a shorter time interval between occurrences were worse prognostic factors. The presence or absence of MPCs had an influence on survival rate according to breast cancer TNM stage. Depending on the site of occurrence of MPCs, breast cancer prognosis varies; thyroid cancer did not affect the prognosis of breast cancer. As a prognostic factor affecting breast cancer survival, MPCs should be considered during follow-up examinations and treatment planning.
 XML Download
XML Download