

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Human epidermal growth factor receptor 2 (HER2) overexpression is observed in approximately 20% of patients with breast cancer, and is associated with a high recurrence rate and poor outcome [1]. Trastuzumab—a humanized monoclonal antibody targeting HER2—has significantly improved clinical outcomes in patients with HER2-positive breast cancer [23]. However, only 20% of patients respond to trastuzumab alone [234], and hence, predictive biomarkers for trastuzumab should be identified in order to maximize its therapeutic benefit.
Mediation of antibody-dependent cell-mediated cytotoxicity (ADCC), which occurs when the monoclonal antibody bound to tumor cells engages with effector cells via the immunoglobulin (Ig) G fragment C receptor (FcrR) expressed on immune cells, is one of the major mechanisms of action of trastuzumab [5]. Genomic FcrR polymorphisms are likely to affect ADCC, and their potential relationship with the clinical outcome of monoclonal antibody therapy has been suggested in lymphoma and colorectal cancer [67], as it influences the affinity of IgG [89]. Although several studies have investigated the role of FcrR polymorphisms in the efficacy of trastuzumab, the findings remain controversial [1011121314].
Moreover, previous studies have shown that lymphocyte infiltration may be correlated with improved survival in several cancer types [151617]. In early stage breast cancer, a greater tumor-infiltrating lymphocytic density, which is mainly found in triple-negative or HER2-positive breast cancer, has been found to be associated with a better response to cytotoxic chemotherapy or HER2-targeted treatment [1819202122232425].
Thus, we aimed to analyze the predictive relevance of FcrR polymorphisms and stromal tumor-infiltrating lymphocyte (sTIL) on the clinical outcome of patients with metastatic HER2-positive breast cancer who received trastuzumab-based chemotherapy.
METHODS
Patients
Between September 2010 and December 2012, 78 patients with metastatic or recurrent HER2-positive breast cancer, who had previously received or were receiving trastuzumab-containing treatment regimens, were enrolled in the present study for analysis of the FcrR3A-158 polymorphism. HER2-positivity was defined by immunohistochemical staining intensity 3+ or 2+/fluorescence in situ hybridization (FISH)-positive. Surgical specimens or biopsy specimens were available for 67 patients (85.9%). As the clinical outcomes could be influenced by the chemotherapy regimens, the study analysis included 56 patients who received the trastuzumab-taxane combination as the first-line treatment for their metastatic or recurrent disease. Although it was not an objective of the original study, we also assessed the sTIL levels in tumor tissues in order to evaluate the potential impact of the level of these cells on clinical outcomes of treatment with the trastuzumab-containing regimen. Data regarding baseline patient characteristics and treatment outcomes were retrospectively obtained by reviewing the patients' medical records. This study was approved by the Institutional Review Board, Asan Medical Center, Seoul, Korea (approval No. 2009-0267), and all patients provided written informed consent.
FcrR3A-158 polymorphism
Blood (2 mL) was collected into ethylenediaminetetraacetic acid tubes and genomic DNA was extracted. FcrR3A genotyping was performed using the single-step multiplex allele-specific real-time polymerase chain reaction techniques previously described [26].
Assessment of stromal tumor-infiltrating lymphocyte level
The sTIL level was retrospectively determined using previously collected formalin-fixed paraffin-embedded tumor tissue acquired from surgery (n=34) or biopsy (n=22). Hematoxylin-and-eosin (H&E)-stained slides were reviewed by breast cancer pathologists who were blinded to the treatment and clinical outcomes. The slides were then histopathologically analyzed for sTIL level, which was defined as the percentage of stroma of invasive carcinoma infiltrated by lymphocytes, based on recommendations of the International TILs Working Group 2014 [27]. For correlative analysis between sTIL and clinical outcomes, patients were classified into high and low sTIL groups (>10% vs. ≤10%) based on the percentage of the tumor stroma containing infiltrating lymphocytes.
Statistical analysis
Tumor responses were determined according to the revised Response Evaluation Criteria in Solid Tumor version 1.1. Progression-free survival (PFS) was defined as the time from the initiation of trastuzumab-taxane chemotherapy until tumor progression or death from any cause, whichever came first. Overall survival (OS) was estimated as the time between the initiation of the trastuzumab-taxane chemotherapy until death from any cause. Survival outcomes were estimated using the Kaplan-Meier method and compared using the log-rank test. Categorical variables were compared using the chi-square or Fisher exact test, as appropriate. A p-value of <0.05 was considered statistically significant, and SPSS version 20.0 (IBM SPSS Inc., Armonk, USA) was used for all statistical analyses.
RESULTS
Patient characteristics
A total of 56 patients included in this analysis received firstline trastuzumab-taxane therapy between June 2006 and March 2013. The median age was 55 years (range, 36–76 years), and all patients had HER2-positive invasive ductal carcinoma. Tumor specimens were found to be positive for the hormone receptor in 33 patients (58.9%), while metastatic disease was initially observed in 19 patients (33.9%). Adjuvant chemotherapy was previously provided to 32 patients (57.1%) and adjuvant trastuzumab after curative surgical resection was administered to nine patients (16.1%). The characteristics of the study population are summarized in Table 1. Overall, the median PFS and OS were 20.0 months (95% confidence interval [CI], 15.0–25.0) and 70.0 months (95% CI, 42.6–97.4), respectively, over a median follow-up duration of 57.0 months (95% CI, 37.4–76.6). A summary of subsequent targeted therapy after progression during treatment with trastuzumab is provided in Supplementary Tables 1 and 2 (available online).
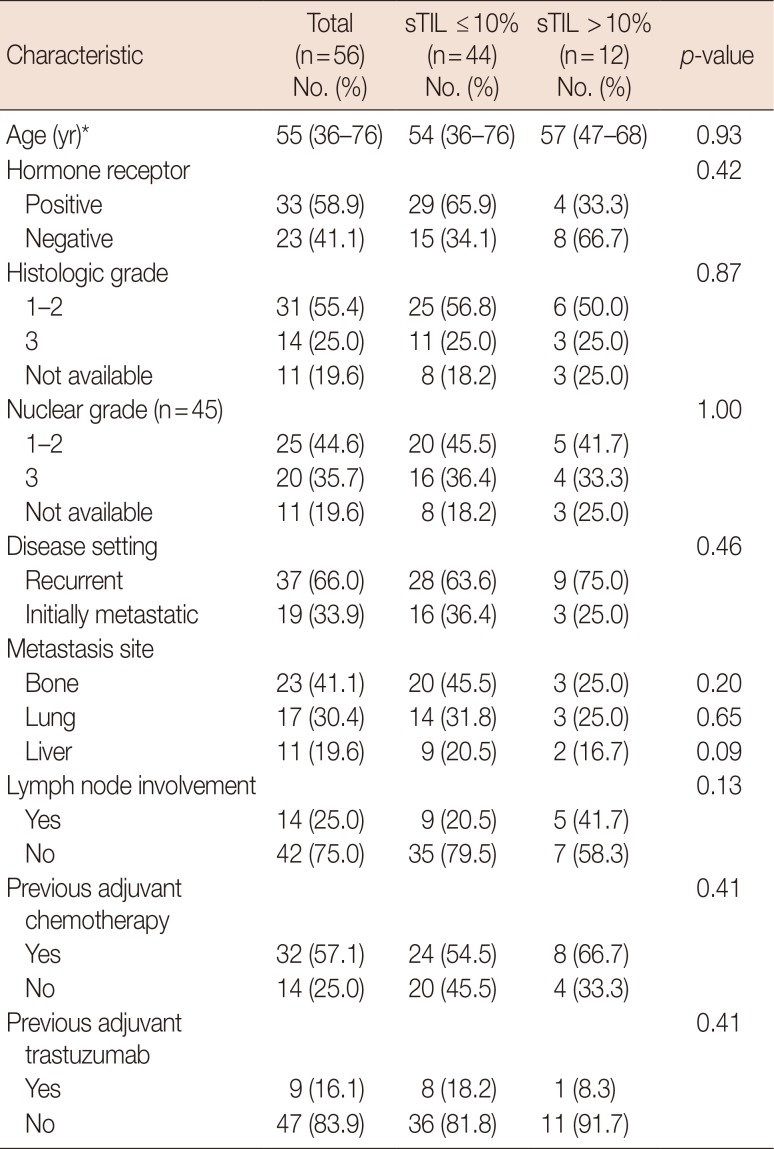
Table 1
Baseline characteristics according to the stromal tumor-infiltrating lymphocyte level
![]()
Correlative analysis for FcrR3A-158 polymorphism
Twenty-three patients (41.1%) were homozygous for the FcrR3A-158 phenylalanine allele (F/F), 23 patients (41.1%) were heterozygous carriers (F/V), and 10 (17.9%) patients were homozygous for the 158 valine allele (V/V). The median PFS and OS were 12.0 months (95% CI, 5.4–18.5) and 46.5 months (95% CI, 24.2–68.7), respectively, in the V/V group, and 22.1 months (95% CI, 12.9–31.3) and 55.1 months (95% CI, 29.0–81.0), respectively, in the F/V group. In the F/F group, the median PFS was 22.9 months (95% CI, 19.5–26.4), and the median OS was 122 months (95% CI, not assessable). The PFS and OS did not differ significantly according to the FcrR3A polymorphism (p=0.32, and p=0.12, respectively) (Figure 1).
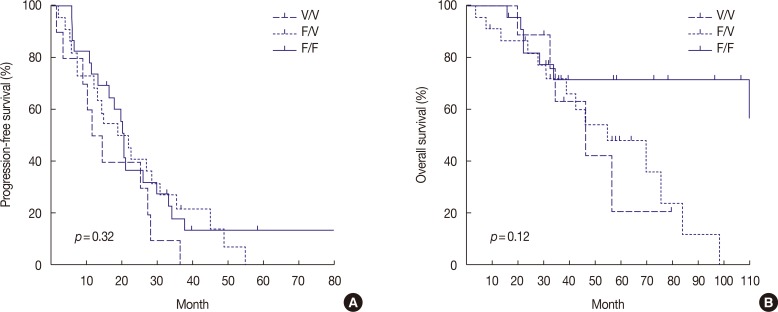
Figure 1
Survival outcomes according to the presence of FcrR3A polymorphisms. Both progression-free survival (A) and overall survival (B) did not differ between the F/F, F/V, and V/V group with p-value of 0.32 and 0.12, respectively.
F/F=phenylalanine/phenylalanine; F/V=phenylalanine/valine; V/V=valine/valine.
![]()
Correlative analysis for stromal tumor-infiltrating lymphocyte
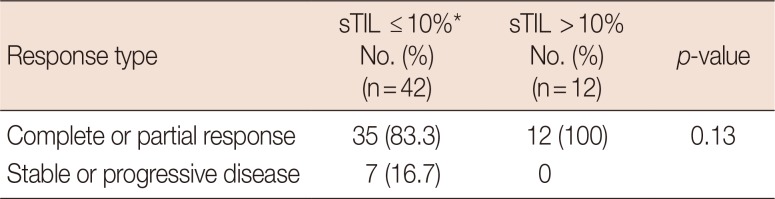
Forty-four patients (78.6%) and 12 patients (21.4%) were assigned to the low and high sTIL groups, respectively. There were no significant differences in age (p=0.93), histologic grade (p=0.87), hormone receptor status (p=0.42), metastatic sites (p>0.05), previous adjuvant chemotherapy (p=0.41), or subsequent targeted therapies between the two groups (p=0.98) (Table 1 and Supplementary Table 1). The median PFS in the high sTIL group (28.4 months; 95% CI, 21.7–35.0) was significantly longer than that in the low sTIL group (16.8 months; 95% CI, 11.1–22.6; p=0.03) (Figure 2). There was no significant difference between the two groups in OS, with a median of 56.9 months (95% CI, 27.3–86.5) in the low sTIL group and 75.9 months in the high sTIL group (95% CI, 22.8–129.0; p=0.58). Among the 54 patients with measurable disease, the objective response rates were 83.3% (35/42) in the low sTIL group and 100% (12/12) in the high sTIL group (Table 2). Although there was a trend toward better response rates in the high sTIL group, this was not statistically significant (p=0.13).
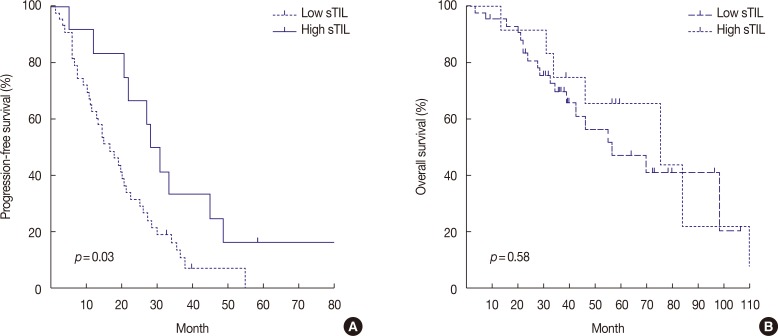
Figure 2
Survival outcomes according to the level of stromal tumor-infiltrating lymphocytes (sTIL). The high sTIL group was significantly associated with a longer progression-free survival (A) compared to the low sTIL group (28.4 months [95% CI, 21.7–35.0] vs. 16.8 months [95% CI, 11.1–22.6]; p=0.03). On the other hand, the high sTIL showed a marginal relationship with better overall survival (B) without statistical significance (vs. low sTIL; 75.9 months [95% CI, 22.8–129.0] vs. 56.9 months [95% CI, 27.3–86.5]; p=0.58).
CI=confidence interval.
![]()
DISCUSSION
Our findings suggest that sTIL level might be a potential predictive marker in patients with metastatic HER2-positive breast cancer treated with trastuzumab-based therapeutic regimens. However, the FcrR3A-158 polymorphism did not appear to be associated with clinical outcomes in patients receiving trastuzumab-based therapy.
In the present study there was a significant association between high sTIL levels and longer PFS in comparison to low sTIL levels (28.4 months vs. 16.8 months, p=0.03) among the 56 patients with metastatic HER2-positive breast cancer who received first-line trastuzumab-taxane chemotherapy. Moreover, the objective response rates of the high sTIL group tended to be higher than those of the low sTIL group (100% vs. 83.3%), although the difference was not statistically significant (p=0.13). While there was no relationship between the sTIL level and OS, this finding might be in part the result of the effects of subsequent treatment after the failure of trastuzumab-taxane therapy, or the small sample size.
The findings of the current study are consistent with the results of previous studies largely performed for early stage breast cancer. In particular, previous retrospective studies on patients with early stage HER2-positive breast cancer who received adjuvant trastuzumab therapy indicated that higher sTIL levels were significantly associated with decreased recurrence rates [2223]. Similar findings were observed in a subanalysis of clinical trials in the neoadjuvant setting [242528]. A previous study based on two large-scale prospective studies—the GeparQuattro and the NeoALTTO trials—concluded that a better pathologic complete response rate was associated with high sTIL levels [2528]. Despite the considerable amount of data on early breast cancer in general, only a few reports to date have described the role of sTILs in advanced breast cancer. Recently, a post hoc analysis of the CLEOPATRA study compared pertuzumab-trastuzumab-docetaxel therapy with placebo-trastuzumab-docetaxel therapy in advanced HER2-positive breast cancer [29]. In the study, in which the sTIL count was evaluated as a continuous variable, higher sTIL levels were significantly associated with improved OS. These findings, in concert with those of the present study, indicate that antitumor immunity may have an impact on the treatment outcomes of advanced stage disease as well as early stage disease.
With regard to the FcrR3A polymorphism, the current study did not show any correlation either with PFS or OS in patients with metastatic HER2-positive breast cancer receiving trastuzumab-based therapy. Although several previous studies have assessed the prognostic significance of FcrR gene polymorphisms in patients with HER2-positive breast cancer treated with trastuzumab, the results have been inconsistent to date [101130]. In a previous retrospective report that included 54 patients with metastatic HER2-amplified breast cancer who received trastuzumab-taxane therapy, both the FcrR3A-158 V/V genotype and FcrR2A-131 H/H genotype were found to be independently associated with a better objective response rate and PFS [10]. A subsequent study also reported that the FcrR2A-131 H/H genotype was significantly associated with better clinical outcomes in patients with both early and metastatic breast cancer [11]; however, the FcrR3A-158 V/V genotype was not correlated with treatment outcome. Furthermore, an analysis of a large patient population (1,286 patients with early stage breast cancer and 53 with metastatic breast cancer) indicated no significant correlation between the FcrR3A or FcrR2A genotypes and the survival outcomes with trastuzumab-based therapy [30].
Evaluation of the predictive ability of sTIL levels in metastatic disease, a topic that has received little investigation in contrast to early breast cancer, is a salient feature of the present study. However, our analysis had several limitations of note. First, this study was performed retrospectively in a small number of patients, and hence, there may be an inherent selection bias in the study population. This factor might explain why patients enrolled in this study showed longer PFS and OS than previously observed. Second, the cutoff point for classifying high sTIL level (>10%) was somewhat arbitrarily determined, as there is currently no available global standard.
In conclusion, the sTIL level may represent a potential predictive biomarker of trastuzumab-based therapy in patients with advanced HER2-positive breast cancer. However, no significant correlation was observed between the FcrR3A polymorphism and clinical outcome. Further investigations should aim to understand the immune microenvironment of HER2-positive breast cancer and standardize the analysis method and clinically relevant cutoff value for categorizing the sTIL status.
 XML Download
XML Download