

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
More than 70% of patients with breast cancer have hormone receptor-positive tumors, resulting in a requirement for endocrine treatment for a period of 5 to 10 years. However, endocrine treatment is not easy to endure for such a long duration owing to the symptoms associated with the drugs used for this treatment. Endocrine treatment-related symptoms are relatively mild, but negatively affect health-related and psychosocial quality-of-life. Symptoms do not fully resolve over the duration of treatment, resulting in increasing nonadherence over the lengthy intervention period [1]. The symptoms increase patient concerns about treatment and their negative beliefs regarding treatment efficacy, also leading to nonadherence [2].
The indication for adjuvant endocrine treatment is clear: women receiving treatment for hormone receptor-positive breast tumors. However, the treatment effect cannot be evaluated before or during treatment. Occasionally, adverse drug effects can be a marker of treatment efficacy. Examples include skin rashes in patients with lung cancer treated with epidermal growth factor receptor inhibitors [3] or hand-foot syndrome in patients with metastatic breast cancer patients treated with capecitabine [4]. In early breast cancer, it is worthwhile to investigate whether endocrine treatment-related symptoms are related to patient survival and can be a predictive marker.
An association between endocrine treatment-related symptoms and patient survival has been suggested previously, and was initially suggested to be associated with tamoxifen metabolism [56]. After the first report, several groups also reported results of exploratory analysis from previous trial data related to this issue [7891011]. However, the results of these studies have been conflicting, making it difficult to draw a conclusion.
In the present study, we performed a meta-analysis of published studies to explore the association between endocrine treatment-related symptoms and patient survival.
METHODS
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [12]. A comprehensive systemic search for published articles was performed using the PubMed, Embase, Scopus, and Cochrane databases, and the last search was performed on December 30, 2015. The main key words used for the search were breast cancer, hormone therapy, endocrine therapy, adverse effects, side effects, and survival. The complete search strategy is presented in the Supplementary Table 1 (available online).
Selection criteria
Studies that met the following criteria were considered for inclusion: all prospective and retrospective studies; studies involving patients with hormone receptor-positive breast cancer who received endocrine treatment for at least 5 years; studies that analyzed the relationship between endocrine treatment-related symptoms and disease recurrence. When duplicate publications were identified, we selected the most comprehensive and recent article. In cases in which only meeting abstracts were available, we contacted the authors to obtain unpublished data.
Data selection and extraction
Eligibility screening and selection for published articles was performed independently by two authors. All full-text articles or meeting abstracts that met the selection criteria were included. Data were also independently abstracted using a data extraction form. The following data were extracted from the published articles: acronym of trial or study, journal, study design, study period, institution, country, endocrine treatment drug type and dosage, method and time point of evaluation of endocrine treatment-related symptoms, definition of endocrine treatment-related symptoms, number of patients, demographic and clinical information of study patients (age, cancer stage), survival outcome, adjustment factors in multivariate analysis, and duration of follow-up. Any disagreement was resolved via reviewer discussion.
When endocrine treatment-related symptoms were evaluated at multiple time points, the latest time point was used for assessment of the primary outcome. In addition, when data from patients with and without baseline symptoms were both reported, results from patients without baseline symptoms were used for determination of the primary outcome.
The risk of bias was systematically evaluated and recorded in a table based on the Risk of Bias Assessment tool for Nonrandomized Studies [13] independently by two reviewers.
Statistical analysis
The primary study aim was to investigate the association between endocrine treatment-related symptoms and recurrence rates. Recurrence rate was obtained in terms of a hazard ratio (HR) of having endocrine treatment-related symptoms. For each study, HRs and 95% confidence intervals (CIs) from multivariate analyses adjusted for confounding factors were extracted from the published article. The adjustment factors for each study are described in the Supplementary Table 2 (available online). Pooled HRs, 95% CIs, and p-values were generated using random-effects modeling. Two-sided p-values less than 0.05 were considered statistically significant. The effects of endocrine treatment-related symptoms on patient survival were also explored based on the type of symptom, specific time-point of symptom evaluation, menopausal status, and baseline symptoms. Studies that did not record baseline symptoms were categorized to include patients with baseline symptoms. Analysis by type of endocrine treatment was not possible owing to insufficient data. Heterogeneity tests were performed using X2 and I2 statistics to quantify the proportion of variability explained by heterogeneity rather than chance. All analyses were performed using STATA version 12.0 (Stata Corp., College Station, USA).
RESULTS
Search and study selection
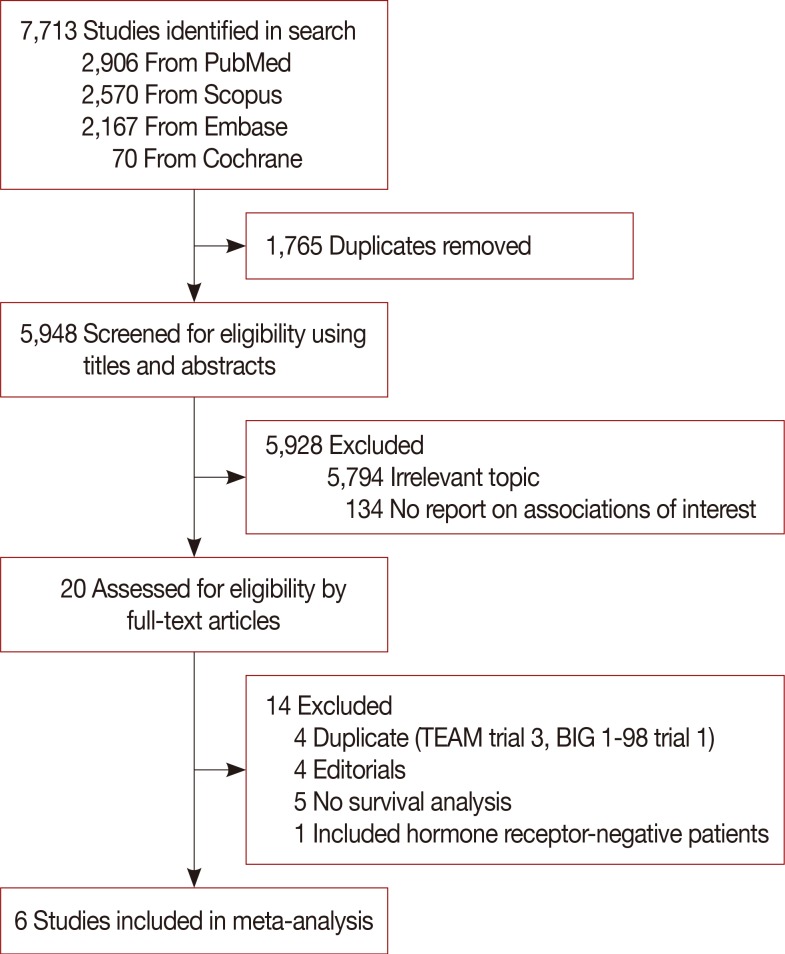
A total of 7,713 articles were identified using the initial search strategy. After removal of duplicates, 5,948 articles were screened by title and abstract. A total of 20 articles were reviewed at the full text level, and six studies meeting the inclusion criteria were ultimately selected for analysis (Figure 1).
Study demographics
The baseline characteristics of the included studies are described in Table 1 and Supplementary Table 2. All included studies enrolled women 18 years or older diagnosed with stage I–III breast cancer, but five studies included only postmenopausal women [7891011]. All studies were exploratory retrospective studies of previous phase 3 trials. Five studies were phase 3 randomized controlled trials comparing endocrine treatment regimens, and one study was a phase 3 randomized controlled trial of the effectiveness of a high-vegetable, low-fat diet [5]. Three studies used recurrence-free survival as a primary outcome [5711], whereas the others used disease-free survival as a primary outcome, including death without disease relapse as an event [8910].
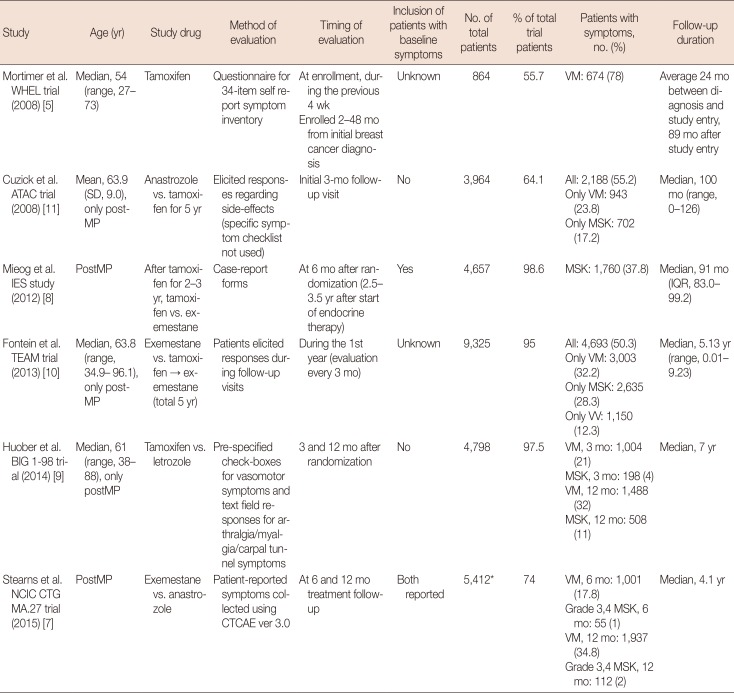
Table 1
Characteristics of the included studies
| Study | Age (yr) | Study drug | Method of evaluation | Timing of evaluation | Inclusion of patients with baseline symptoms | No. of total patients | % of total trial patients | Patients with symptoms, no. (%) | Follow-up duration |
|---|---|---|---|---|---|---|---|---|---|
| Mortimer et al. WHEL trial (2008) [5] | Median, 54 (range, 27–73) | Tamoxifen | Questionnaire for 34-item self report symptom inventory | At enrollment, during the previous 4 wk | Unknown | 864 | 55.7 | VM: 674 (78) | Average 24 mo between diagnosis and study entry, 89 mo after study entry |
| Enrolled 2–48 mo from initial breast cancer diagnosis | |||||||||
| Cuzick et al. ATAC trial (2008) [11] | Mean, 63.9 (SD, 9.0), only postMP | Anastrozole vs. tamoxifen for 5 yr | Elicited responses regarding side-effects (specific symptom checklist not used) | Initial 3-mo follow-up visit | No | 3,964 | 64.1 | All: 2,188 (55.2) | Median, 100 mo (range, 0–126) |
| Only VM: 943 (23.8) | |||||||||
| Only MSK: 702 (17.2) | |||||||||
| Mieog et al. IES study (2012) [8] | PostMP | After tamoxifen for 2–3 yr, tamoxifen vs. exemestane | Case-report forms | At 6 mo after randomization (2.5–3.5 yr after start of endocrine therapy) | Yes | 4,657 | 98.6 | MSK: 1,760 (37.8) | Median, 91 mo (IQR, 83.0–99.2) |
| Fontein et al. TEAM trial (2013) [10] | Median, 63.8 (range, 34.9–96.1), only postMP | Exemestane vs. tamoxifen → exemestane (total 5 yr) | Patients elicited responses during follow-up visits | During the 1st year (evaluation every 3 mo) | Unknown | 9,325 | 95 | All: 4,693 (50.3) | Median, 5.13 yr (range, 0.01–9.23) |
| Only VM: 3,003 (32.2) | |||||||||
| Only MSK: 2,635 (28.3) | |||||||||
| Only VV: 1,150 (12.3) | |||||||||
| Huober et al. BIG 1-98 trial (2014) [9] | Median, 61 (range, 38–88), only postMP | Tamoxifen vs. letrozole | Pre-specified check-boxes for vasomotor symptoms and text field responses for arthralgia/myalgia/carpal tunnel symptoms | 3 and 12 mo after randomization | No | 4,798 | 97.5 | VM, 3 mo: 1,004 (21) | Median, 7 yr |
| MSK, 3 mo: 198 (4) | |||||||||
| VM, 12 mo: 1,488 (32) | |||||||||
| MSK, 12 mo: 508 (11) | |||||||||
| Stearns et al. NCIC CTG MA.27 trial (2015) [7] | PostMP | Exemestane vs. anastrozole | Patient-reported symptoms collected using CTCAE ver 3.0 | At 6 and 12 mo treatment follow-up | Both reported | 5,412* | 74 | VM, 6 mo: 1,001 (17.8) | Median, 4.1 yr |
| Grade 3,4 MSK, 6 mo: 55 (1) | |||||||||
| VM, 12 mo: 1,937 (34.8) | |||||||||
| Grade 3,4 MSK, 12 mo: 112 (2) |
![]()
The method of evaluating endocrine treatment-related symptoms varied among studies. Three studies exclusively used a standardized method [579], and the other studies reported results from elicited symptoms or patient responses [891011]. The time point of symptom evaluation also differed among studies. Three studies had specific time points of evaluation: 3, 6, and 12 months after the start of treatment [7911]. Two studies also had specific time points, but the time of trial entry varied among patients [58]. One study included all patients who reported endocrine treatment-related symptoms during the first year after the start of treatment [10]. All studies reported results of multivariate analysis regarding the recurrence rate according to endocrine treatment-related symptoms. In one study, the author was directly contacted to obtain specific HRs and 95% CIs [7].
Vasomotor symptoms were defined as hot flashes and night sweats in all studies. One study [9] included vaginal dryness in the vasomotor symptom category. Most studies included joint symptoms and muscle symptoms as musculoskeletal symptoms, with the exception of one study [11] that included only joint symptoms, such as arthralgia and arthritis, in this category. The definitions of musculoskeletal symptoms varied between studies; these are summarized in Table 1. The inclusion of patients with baseline vasomotor or musculoskeletal symptoms differed among studies. Two studies [911] included only patients with no baseline symptoms, one study [8] included patients with baseline symptoms, and two other studies [510] did not record whether patients had baseline symptoms. In addition, one study [7] reported data for patients both with and without baseline symptoms.
Meta-analysis
The results of the risk of bias assessment are described in the Supplementary Table 3 (available online). The funnel plot is also presented in the Supplementary Figure 1 (available online).
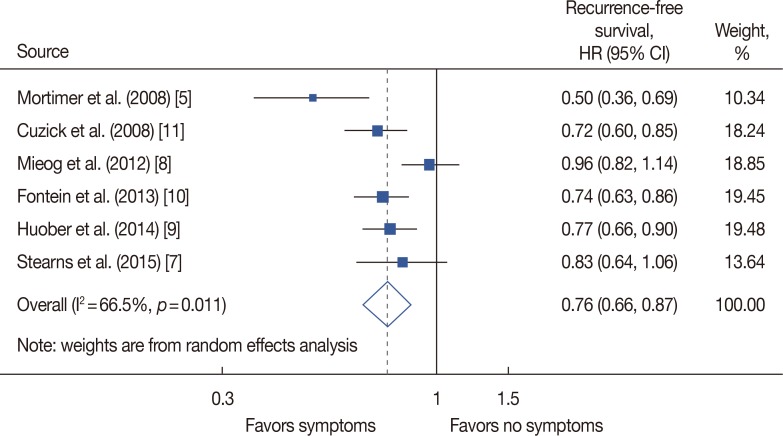
The pooled model revealed a significantly lower recurrence rate for patients who developed any endocrine treatment-related symptoms compared with patients with no related symptoms (HR, 0.76; 95% CI, 0.66–0.87) (Figure 2). Study heterogeneity was statistically significant (I2=66.5%) but this result was largely due to the inclusion of a small study [5] from a dietary trial.
For patients who had only vasomotor symptoms, the HR was 0.74, compared with patients without any symptoms (95% CI, 0.63–0.87; four studies) (Figure 3A). Patients who reported only musculoskeletal symptoms also had a lower recurrence rate than patients with no symptoms (HR, 0.69; 95% CI, 0.55–0.86; three studies) (Figure 3B). Substantial study heterogeneity was shown in both of these analyses as well (I2= 65.7%, p=0.033; I2=69.8%, p=0.036, respectively).
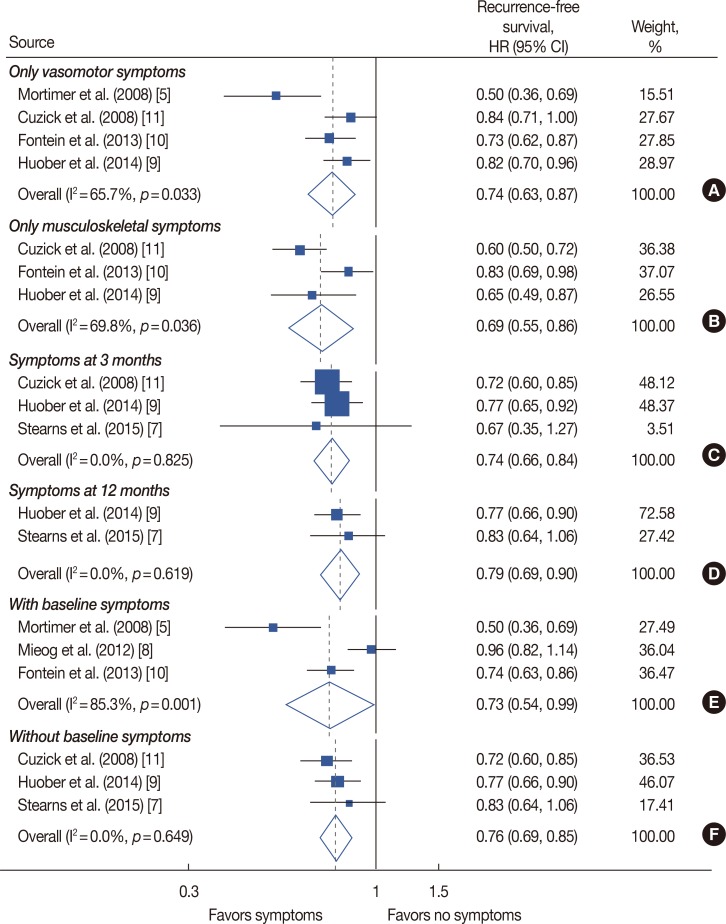
Figure 3
Meta-analysis of endocrine treatment-related symptoms and recurrence-free survival according to type of symptom, time point of symptom evaluation and inclusion of patients with baseline symptoms. Forest plot for patients with only vasomotor symptoms (A) and patients with only musculoskeletal symptoms (B). Forest plot according to evaluation time point by specific time point of 3 months (C) and 12 months (D) after start of treatment. (E) Meta-analysis result when including patients with baseline symptoms. (F) Forest plot of only including patients with no baseline symptoms.
HR=hazard ratio; CI=confidence interval.
![]()
When data were pooled according to the time point of symptom evaluation, significantly lower recurrence rates were noted in patients with endocrine treatment-related symptoms than in patients reporting no related symptoms at the specific time points of 3 months and 12 months (HR, 0.74, 95% CI, 0.66–0.84, three studies; HR, 0.79, 95% CI, 0.69–0.90, two studies, respectively) (Figure 3C and D).
Heterogeneity was low for both analyses of time point of symptom evaluation (I2=0.0%, p=0.825; I2=0.0%, p=0.619, respectively).
For studies including patients with baseline symptoms, patients with endocrine treatment-related symptoms exhibited a lower recurrence rate than patients with no symptoms (HR, 0.73; 95% CI, 0.54–0.99; three studies) (Figure 3E). In this analysis, study heterogeneity was quite substantial (I2=85.3%, p=0.001). Similar results were demonstrated in a pooled analysis for three studies that included only patients with no baseline symptoms (HR, 0.76; 95% CI, 0.69–0.85) (Figure 3F).
In five studies that included only postmenopausal women, the HR was 0.80 for patients with endocrine treatment-related symptoms compared with patients with no related symptoms (95% CI, 0.72–0.89) (Supplementary Figure 2, available online). Study heterogeneity was moderate in this analysis (I2=45.7%, p=0.118).
DISCUSSION
This systematic review and meta-analysis demonstrated that patients with breast cancer who experienced endocrine treatment-related symptoms had a lower recurrence rate than patients who did not report these symptoms. This relationship persisted despite type of symptoms (vasomotor symptoms and musculoskeletal symptoms), time point of symptom evaluation (3 months or 12 months after initiation of endocrine treatment), inclusion of patients with baseline vasomotor or musculoskeletal symptoms, or exclusive inclusion of postmenopausal women. All analyses revealed similar HRs of 0.69 to 0.80.
The efficacy of adjuvant endocrine treatment has been repeatedly proven in breast cancer. However, owing to the long duration of adjuvant treatment, adherence is an important concern. The association of low adherence with lower patient survival enhances the significance of this relationship [14]. The reported rates of early discontinuation of endocrine treatment in the trials included in this study were 8.1% to 31.6% [1516]. However, in nonclinical trial settings, the treatment discontinuation rate increases to 31% to 73%; thus, greater than two-thirds of survivors did not complete 5 years of adjuvant endocrine treatment [1718]. One of the strongest and most consistent risk factors for low treatment adherence is endocrine treatment-related symptoms [1419]. Another recognized risk factor is a patient's negative beliefs regarding treatment efficacy [220]. The results of this study can be used in clinical practice and serve as a reference for changing patient negative beliefs, especially in the case of patients suffering from side effects of endocrine therapy, into positive beliefs. This information is also encouraging to patients and physicians enduring these symptoms over a period of at least 5 years.
The reported rate of symptoms varied among included trials: 23.8% to 78% for vasomotor symptoms and 11% to 37.8% for any musculoskeletal symptoms. The various evaluation methods and time points used in the included studies caused this wide range of prevalence and also contributed to study heterogeneity in several analyses. The reported rate was higher when a specific checklist or questionnaire was used or when patients with baseline symptoms were included (Table 1). Previous trials that did not use protocol-based standardized evaluation methods have been reported to underestimate the prevalence of endocrine treatment-related symptoms [2122]. In addition, the reported rate of musculoskeletal symptoms was lower in the trials included in this meta-analysis compared with more recent studies [2123]. The trials included in this meta-analysis were conducted in the late 1990s to early 2000s, when adverse events related to aromatase inhibitors were not well known. This limitation might have led to underestimation of symptom prevalence.
Statistically significant heterogeneity was demonstrated in several analyses in the present study. In the primary analysis, the main source of heterogeneity was the WHEL study [5]. This study was the only study not comparing endocrine treatment drugs and the only study that included premenopausal women. A wide symptom evaluation period of 2 to 48 months after diagnosis may also have contributed to study heterogeneity. The ATAC trial [11] also featured a wide period of evaluation (during the first year of endocrine treatment), leading to significant heterogeneity in the analysis for musculoskeletal symptoms and recurrence rate.
The mechanism underlying the relationship between endocrine treatment-related symptoms and improved survival remains unclear. Vasomotor symptoms are generally thought to be the result of decreased estrogen and related to the thermoregulatory set-point [24]. Therefore, the association of vasomotor symptoms with treatment efficacy can serve as a rational approach. More severe hot flashes in patients with lower estradiol levels have been previously observed, supporting this hypothesis [25]. The etiology of endocrine treatment-related musculoskeletal symptoms is more obscure, and several hypotheses have been reported. Estrogen deprivation, antinociceptive effects, joint effusion, and autoimmunity are some of the possible sources of musculoskeletal symptoms [2627]. Connecting these causes to the association between musculoskeletal symptoms and improved survival with endocrine therapy will require additional studies. The use of pharmacological interventions to ease these symptoms should also be considered when investigating this relationship [28].
Despite this variety of approaches and evidence, the link between endocrine treatment-related symptoms and treatment efficacy may be simply the result of differences in adherence. In the ATAC trial [11], a nonsignificant increase in patient drug adherence was observed in patients reporting symptoms (88%) compared with those with no symptoms (84%). Physical symptoms are only recorded when patients report them, and a hypothesis that patients reporting their symptoms might be more likely to take their pills than those who do not report symptoms is a possible explanation. However, endocrine treatment-related symptoms are well-known risk factors for nonadherence, and other studies also report higher rates of symptoms in nonadherent patients [29], challenging this hypothesis.
We encountered several limitations during this study. The meta-analysis included a small number of studies, and substantial heterogeneity was noted among them. High-quality summarization was difficult and careful interpretation of our results is necessary. Confounding factors were adjusted by taking recurrence rate data from multivariate analysis of each study, but interpretation is limited as the adjustment factors differed among studies. Most of the studies included in this meta-analysis evaluated endocrine treatment-related symptoms by patient report, not by checklists, resulting in a lower rate of adverse effects compared to previous literature. Also, the time point of symptom evaluation and inclusion/exclusion of patients with baseline symptoms differed in each study, resulting in differences in the proportion of patients with symptoms among studies. Patients who experienced recurrence before the time point of evaluation were excluded in each study, which also may have led to possible bias in the results. Subgroup analysis according to endocrine treatment type or drug was not possible, and it remains unclear whether the prognostic influence of endocrine treatment-related symptoms is for all drugs or only for specific drugs. Most of the included studies were trials comparing aromatase inhibitors with tamoxifen, or studies that only involved postmenopausal women. Extending the results of this study to premenopausal women will require further evaluation.
Confirming endocrine treatment-related symptoms as a predictive marker of endocrine treatment still requires careful consideration. To accurately identify a predictive marker, a study with a placebo or no treatment group is needed [330]. However, considering that endocrine treatment is the standard treatment for patients with hormone receptor-positive breast cancer, a clinical trial in that setting is practically impossible. At minimum, a uniform evaluation method along with a standardized patient-reported outcome will be required for accurate determination of symptoms and their relationship with patient survival.
In conclusion, the results of this meta-analysis demonstrate that endocrine treatment-related symptoms are related to lower recurrence in patients with breast cancer, especially in postmenopausal women. This information can be used as guidance for clinical advice and serve as motivation for patients to continue taking medication.
 XML Download
XML Download