

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
More patients with breast cancer are being diagnosed at early stages; however, the incidence of total mastectomy (TM) has not decreased accordingly in Korea [1]. This trend is related to the increasing popularity of immediate breast reconstructions (IBR), and the use of prophylactic contralateral mastectomy rather than breast-conserving surgery (BCS) in BCS-eligible patients has increased [23]. Moreover, this trend of IBR in Korea is expected to further increase because the Korean National Health Insurance System began covering breast reconstructions in patients with breast cancer in April 2015.
Since Toth and Lappert [4] first introduced skin-sparing mastectomy (SSM) in the 1990s, SSM has yielded oncologic outcomes similar to those of TM with higher levels of patient satisfaction and quality of life [56]. Success with SSM has paved the way for nipple-sparing mastectomy (NSM) in selected patients with breast cancer. Although IBR following SSM and NSM is popular, the oncologic safety and surgical outcomes remain controversial.
Recently, it has become more difficult to compare the oncologic safety between such methods; this is because more patients are choosing IBR following TM even though they were BCS-eligible and the indications for IBR have been expanded to include those with advanced breast cancer, close tumor-nipple distance, neoadjuvant chemotherapy (NAC), and postmastectomy radiation therapy who underwent IBR [278910]. This study sought to analyze the oncologic outcomes between TM only and IBR following NSM or non-NSM (NNSM) in a population matched by age at operation, year of operation, pathologic stage, estrogen receptor (ER)/progesterone receptor (PR) status, and human epidermal growth factor receptor 2 (HER2) status.
METHODS
Data of the patients with breast cancer who underwent TM were collected retrospectively between January 2008 and December 2014 at Samsung Medical Center in Seoul, South Korea. We excluded patients who underwent NAC, including palliative chemotherapy, had a follow-up duration <12 months, experienced inflammatory breast cancer, and with incomplete data. Patients were divided into two groups: TM only (control group) and IBR following NSM/NNSM (study group). Both groups were matched by propensity scores maximally (1:2). Matched variables included age at operation, year of operation, pathologic stage, ER/PR status, and HER2 status. We collected clinicopathologic and surgical data via an electronic medical chart review.
Locoregional recurrence (LRR) was defined as a local recurrence (tumor recurrence within the ipsilateral chest wall [skin, subcutaneous tissue, and pectoralis muscle]) or regional recurrence (recurrence in the ipsilateral axillary, supraclavicular, internal mammary, or infra-clavicular lymph nodes [LN]). Distant metastasis (DM) was defined as any recurrence in other areas not included in LRR. Data on recurrence events were collected via a review of electronic medical records, and survival data were acquired from electronic medical records as well as the Korean National Statistical Office database. Pathologic staging followed the seventh American Joint Committee on Cancer classification [11]. Adjuvant chemotherapy and radiotherapy were performed as recommended by the dedicated medical oncologist and radiologist. TM including NSM and NNSM was performed by a breast surgeon and IBR by a plastic surgeon. The type of breast reconstruction was determined during preoperative consultation with the plastic surgeon in accordance with the patient's physical presentation and preference. This study adhered to the ethical tenets of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Samsung Medical Center (IRB number: 2015-07-103-003). The need for informed consents was waived because of the retrospective nature of this study.
Statistics
Patient characteristics were compared using weighted independent t-tests for continuous variables and weighted chi-square or Fisher exact tests for categorical variables. Kaplan-Meier curves, with corresponding log-rank tests, were constructed for overall survival (OS), disease-free survival (DFS), distant metastasis-free survival (DMFS), and locoregional recurrence-free survival (LRFS) rates. The primary endpoint was DFS. For all analyses, a p-value <0.05 was considered statistically significant. Univariate and multivariate analyses for DFS were conducted with Cox regression for clustered-matched data. Multivariate analysis was conducted if the p-value was <0.200 in the univariate analysis. All statistical analyses were executed using the SAS version 9.4 (SAS Institute, Cary, USA) and R version 3.2.5 (Vienna, Austria; http://www.R-project.org).
RESULTS
Study design
The study design is shown in Figure 1. Among the patients who underwent TM for breast cancer between January 2008 and December 2014, we excluded patients who underwent NAC (n=309), those with a follow-up duration <12 months (n=147), those with incomplete data (n=24), and those who underwent palliative surgery (n=11). After propensity score matching, 878 patients were included in the control group and 580 patients in the study group.
Patient characteristics
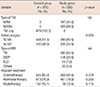
The basic characteristics of the control and study groups are shown in Table 1. The median follow-up duration was 43.4 months (range, 11–100 months) for the control group and 41.3 months (range, 12–100 months) for study group (p=1.000). The mean age was 47.3±8.46 years for the control group and 43.9±7.14 years for the study group (p>0.050). There were no significant differences between the control and study groups in the matching variables or in family history, histopathology, multiplicity, and presence of lymphovascular invasion (LVI). Only nuclear grade (NG) and body mass index varied significantly between the two groups.
Type of surgical and adjuvant treatments
Surgical and adjuvant treatments are summarized in Table 2. In the study group, 197 patients (34.0%) underwent NSM, and 383 patients (66.0%) underwent NNSM. Among them, 380 patients (65.5%) underwent tissue expander insertion, 146 (23.5%) underwent deep inferior epigastric perforator flap creation, and 44 (7.6%) underwent extended latissimus dorsi flap creation. More patients in the study group underwent sentinel LN biopsy only than in the control group (p=0.003). In the control and study groups, 525 (60.0%) and 293 (50.5%) patients received adjuvant chemotherapy, respectively, while 167 (19.1%) and 78 (13.5%) received adjuvant radiotherapy, respectively. There was no significant difference in hormonal therapy between the two groups (p=0.203).
Oncologic outcomes
In the control group, 16 patients had LRR, 32 patients had DM, and four patients expired. In the study group, 18 patients had LRR, 14 patients had DM, and four patients expired (Table 3). There was no significant difference in OS (log-rank p=0.454), DFS (log-rank p =0.186), DMFS (log-rank p=0.537), or LRFS (log-rank p=0.114) (Figure 2). In the multivariate analysis, there was no significant difference in DFS between the two groups (p=0.058) (Table 4). Subgroup analysis of the study group revealed no significant differences in OS (log-rank p=0.777), DFS (log-rank p=0.274), DMFS (log-rank p=0.085), or LRFS (log-rank p=0.293) (Figure 3). NSM also did not show significant differences when compared to NNSM (p=0.363) (Table 4).
Complications
There were no significant differences between the two groups in complication rates (p=0.762). Five cases in the study group experienced complications: two cases of partial skin necrosis, one of nipple excision due to nipple necrosis, and two of postoperative bleeding. There were six cases with complications in the control group: four cases of postoperative bleeding and two of partial skin necrosis.
DISCUSSION
The number of patients who underwent IBR following NSM and NNSM has increased in recent years. However, concerns remain regarding oncologic outcomes, and the National Comprehensive Cancer Network recommends IBR following NSM and NNSM only for selected patients treated by experienced multidisciplinary teams [12]. In this study, there were no significant differences in DFS, LRFS, DMFS, or OS between the control and study groups after propensity matching by age at operation, year of operation, pathologic stage, ER/PR status, and HER2 status.
Several studies have reported no difference in oncologic outcomes between TM only and IBR following NSM/NNSM [1314151617]. Platt et al. [18] reported that the oncologic outcomes of breast reconstruction did not vary in the TM only group in the Ontario Cancer Registry, which included 758 breast reconstruction and 1,516 control patients matched by age and cancer histology among the total 13,888 patients with breast cancer. The median follow-up duration in that study was 23.4 years. Petit et al. [19] compared 518 patients who underwent IBR following TM with 159 patients who underwent TM only. The follow-up duration was 70 months (range, 15–114 months). They reported no difference in OS or DFS between the two groups. Jeon et al. [20] also reported a 5-year LRFS rate for NSM and NNSM of 92.1 and 95.2, respectively, suggesting that IBR following NSM and NNSM is an oncologically safe procedure (p>0.05).
However, whether IBR following NSM/NNSM affects the prognosis of breast cancer remains controversial. There are many selection biases with regard to IBR in oncologic favorable situations [20212223]. Wu et al. [24] demonstrated using Surveillance, Epidemiology, and End Results (SEER) data that patients with HER2 overexpressing overexpression or triple-negative breast cancer (who have a relatively higher risk of local recurrence) were less likely to undergo IBR than those with luminal subtype tumors. Another study using SEER data including 54,660 patients with breast cancer showed an improved cancer-specific survival rate (BCSS) (hazard ratio, 0.47; 95% confidence interval, 0.28–0.80) [25]. However, the IBR group included oncologically favorable characteristics as follows: early-stage breast cancer (stage I, 39.6% vs. 34.5%, p<0.0001), ER positivity (65.4% vs. 63.8%, p<0.0001), PR positivity (54.9% vs. 52.0%, p<0.0001), and no LN metastasis (N0, 56.1% vs. 52.6%, p<0.0001). Petit et al. [19] also showed a patient selection bias in the IBR group, which included younger patients (<35 years, 94.2% vs. 5.8%, p<0.001), smaller tumors (pT1, 86.7% vs. 13.3%, p<0.001), no LN metastasis (N0, 79.8% vs. 20.2%, p<0.001), ER positivity (74.1% vs. 25.9%, p<0.001), PR positivity (74.1% vs. 25.9%, p<0.001), and low NG (G1, 85,6% vs. 14.4%, p=0.017). Age, stage, ER/PR status, and HER2 status could affect the oncologic outcome. Therefore, well-designed studies with populations matched by age, stage, ER/PR status, and HER2 status are needed.
There have been a few matched case-control studies. Eriksen et al. [26] reported a retrospective cohort matched by age, tumor size, nodal stage, and year of operation (between 1990 and 2004). The median follow-up duration was 11.5 years. LRR was not significantly different between the groups (8.2% in the IBR group and 9.0% in the TM only group, p=0.879). The IBR group showed better OS and BCSS than the TM only group (p=0.038 and p=0.026, respectively). This study was well designed with a long-term follow-up. However, more ER/PR positive patients were enrolled in the IBR group, and the HER2 status could not be identified. Disproportionate hormonal status and unknown HER2 status may affect the OS and BCSS. Recently, Park et al. [27] compared the oncologic outcomes between TM only and IBR following TM in a population matched by age, tumor size, axillary LN metastasis, and ER status between 2002 and 2010. The median follow-up duration was 65.6 months (range, 10–132 months) in the IBR group and 81.1 months (range, 1–154 months) in the TM only group (p<0.001). DFS and LRFS were not significantly different between the two groups (p=0.496 and p=0.704, respectively). This study was also well designed; patients were matched by tumor size, LN metastasis, ER/PR status, and Ki-67 score. However, the difference in follow-up duration could have led to a time bias. Furthermore, more young patients (22.8% vs. 13.8%, p=0.003) and less HER2-amplified patients (59.8% vs. 72.1%, p=0.005) were enrolled, which could have affected the recurrence. In the present study, matching was considered successful for the matching variables as well as other potentially associated factors, such as family history, histology, multiplicity, and LVI. Furthermore, our study showed concurrent results with those of other matched case-control studies.
Our study has a few limitations. It was a retrospective study; therefore, selection bias may be an issue. Although all tested factors were matched successfully, a low NG was more prevalent in the study group (18.8% vs. 14.4%, p=0.027). The follow-up duration was also relatively short for comparing long-term outcomes. Lastly, we could not quantify the Ki-67 score, which could affect the recurrence.
In conclusion, IBR following NSM or NNSM could be a feasible surgical treatment option for breast cancer. In future studies, a larger study population with a long-term follow-up is needed to more accurately determine oncologic outcomes.






 XML Download
XML Download