

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer-related death in women, accounting for 25% of all female cancers, and 14% of cancer-related deaths globally [1]. In Korean women, breast cancer is the second most common type of cancer, and the incidence rate has been rising [23]. According to data from the Korean Breast Cancer Society registry, the median age of diagnosis of breast cancer was 50 years, and the proportion of patients older than 70 years was estimated at about 7% [3]. A rapid increase in the size of the elderly population has resulted in a concomitant increase in the number of diagnosed cases of breast cancer in elderly women [34]. Evidence exists to show that breast cancer incidence and mortality rates increase with age. According to the National Cancer Institute Surveillance, Epidemiology, and End Results Cancer Statistics Review, 43% of patients with newly diagnosed breast cancers were aged ≥65 years and 20% were aged ≥75 years, and a majority of the breast cancer mortalities occurred in these age groups [5].
As the incidence of elderly breast cancer is increasing, the absolute number of elderly patients with metastatic disease is also on the rise. Irrespective of the patient's age, metastatic breast cancer (MBC) is incurable, and approximately 25% of all patients diagnosed with MBC survive for 5 years [2]. While the process for diagnosing and treating MBC in younger patients is well-defined, the principles of treatment are relatively not well established in elderly patients because of under-representation of this age group in clinical trials [678]. Modified management strategies are often used for older individuals; however, supporting evidence for such approaches is poor, and often leads to under-treatment, which has been well documented in several studies [910]. Chemotherapy, which can be associated with substantial toxicity, is usually indicated in elderly patients with hormone receptor (HR)-negative disease, hormone-refractory disease, or rapidly progressing disease. The elderly population possesses variability in physical, cognitive, and psychosocial function; some may tolerate chemotherapy as well as younger patients, while others may experience unpredictable and severe side effects [1112]. Thus, for elderly patients, it is important to customize therapy using parameters based on a geriatric assessment, and such parameters need to be evaluated through prospective clinical trials [1314]. Currently, there is little information regarding the potential risks and benefits associated with treatment for MBC in elderly patients, as only a few studies have focused directly on these patients. In this regard, in order to increase our knowledge on optimal clinical care of these patients, and to gain important insights into well-designed prospective clinical trials focusing on the specific requirements of elderly patients, it is important that we understand how these patients are currently being treated in real-world clinical practice.
In this retrospective study, we examined a cohort of elderly patients with MBC, receiving a range of treatments at three academic hospitals in South Korea. We analyzed demographic and clinicopathologic characteristics, treatment patterns, and treatment outcomes, to understand underlying correlations between parameters.
Go to : 
METHODS
Study population
Patients aged ≥65 years diagnosed with MBC between 2003 and 2015 were identified from the databases of three academic hospitals in South Korea. We reviewed and analyzed the characteristics of the patients who met the following inclusion criteria: patients with a history of either recurrent breast cancer or those presenting with de novo stage IV disease, patients with no previous history of treatment for metastatic disease, and patients aged ≥65 years. Recurrent breast cancer did not include cases of isolated ipsilateral or contralateral breast recurrence, isolated regional lymph node recurrence, or that of local chest wall recurrence. The date of recurrence was defined as the time of detection of first distant metastasis. Treatments for MBC were administered according to standard-of-care by the treating oncologist.
A total of 161 cases were identified, and we assessed the clinicopathologic features, treatment patterns, and follow-up treatment outcomes using our available electronic medical records. Patients were divided into three comparison groups based on age at MBC diagnosis: 65 to 69 years, 70 to 74 years, and ≥75 years.
This study was approved by the Institutional Review Board of Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University Hospital, and Seoul National University Bundang Hospital (IRB numbers: 16-2016-31, J-1612-002-809, and B-1606-349-114), respectively. In this retrospective outcomes study, the informed consent was waived.
Data collection
Data were extracted for the following variables: (1) baseline demographics and clinicopathologic information such as patient's age, performance status (PS), comorbidities, estrogen receptor (ER) and progesterone receptor (PR) status, human epidermal growth factor receptor 2 (HER2) status, metastatic sites and number; (2) details of treatment with chemotherapy, hormonal therapy, surgery, and radiation therapy; and (3) surveillance information including date of last visit or follow-up, date of recurrence (in case of distant recurrence after primary surgery), and survival status.
The Charlson comorbidity index (CCI) was assessed based solely on the retrospective review of the patient's medical records.
The data pertaining to HR and HER2 status, as ascertained by immunohistochemical analysis, was obtained from medical records, and analyzed. The tumor tissues were evaluated for ER and PR status by standard immunohistochemistry, and tumors were considered receptor-positive if at least 1% of cells tested were stain-positive. The HER2 status was also evaluated by immunohistochemistry staining, and tumors were considered receptor-positive if the staining intensity was 3+. The staining intensity of zero or 1+ were considered receptor-negative and the intensity of 2+ were further evaluated with fluorescence in situ hybridization.
Statistical analysis
Descriptive analyses were performed to evaluate clinicopathologic characteristics and treatment modalities. Data were stratified by age (65–69 years, 70–74 years, and ≥75 years), and descriptive statistics were employed to examine differences between the strata. Categorical variables were compared using the chi-square test or the Fisher exact test. Some of the measures required a log transformation in order to meet the normality assumptions. Survival curves, estimated by the Kaplan-Meier method, were compared across groups using the log-rank method. Overall survival (OS) was measured from the first diagnosis of MBC to the date of death from all causes or last follow-up date. For multivariate analysis, a Cox proportional hazards regression model was used to estimate the adjusted hazard ratio for determining the significance of prognostic factors. All analyses were carried out using the IBM SPSS Statistics version 20.0 (IBM Corp., Armonk, USA) software. The statistical significance was set at p<0.05.
Go to :
RESULTS
Patient characteristics
A total of 161 patients with a median age of 71 years (range, 65–86 years) were identified. The distribution of patients by age group was as follows: 65 to 69 years (n=54, 33.5%); 70 to 74 years (n=67, 41.6%); and ≥75 years (n=40, 24.8%). The baseline demographic and clinicopathologic information of patients is summarized in Table 1. The majority of patients had Eastern Cooperative Oncology Group (ECOG) PS of 0–1. Thirty percent of patients in the ≥75 years group had an ECOG PS ≥2 as compared to 10.4% of those in the 70 to 74 years group, and 9.3% of those in the 65 to 69 years group (p=0.005). The highest CCI score ≥11 was exhibited by 100% of patients aged ≥75 years, while, in comparison, this score was seen in 73.1% of those aged 70 to 74 years, and in 3.7% of those aged 65 to 69 years (p<0.001). Among the patients tested, an ER and/or PR positive status was seen in 61.5% of patients, and a HER2 positive status was seen in 24.2% of patients. There were no significant differences in HR positivity and HER2 overexpression status across age groups. The HER2 status was less frequently tested among patients ≥75 years. Approximately 40% of patients had de novo stage IV disease and 60% had recurrent breast cancer.
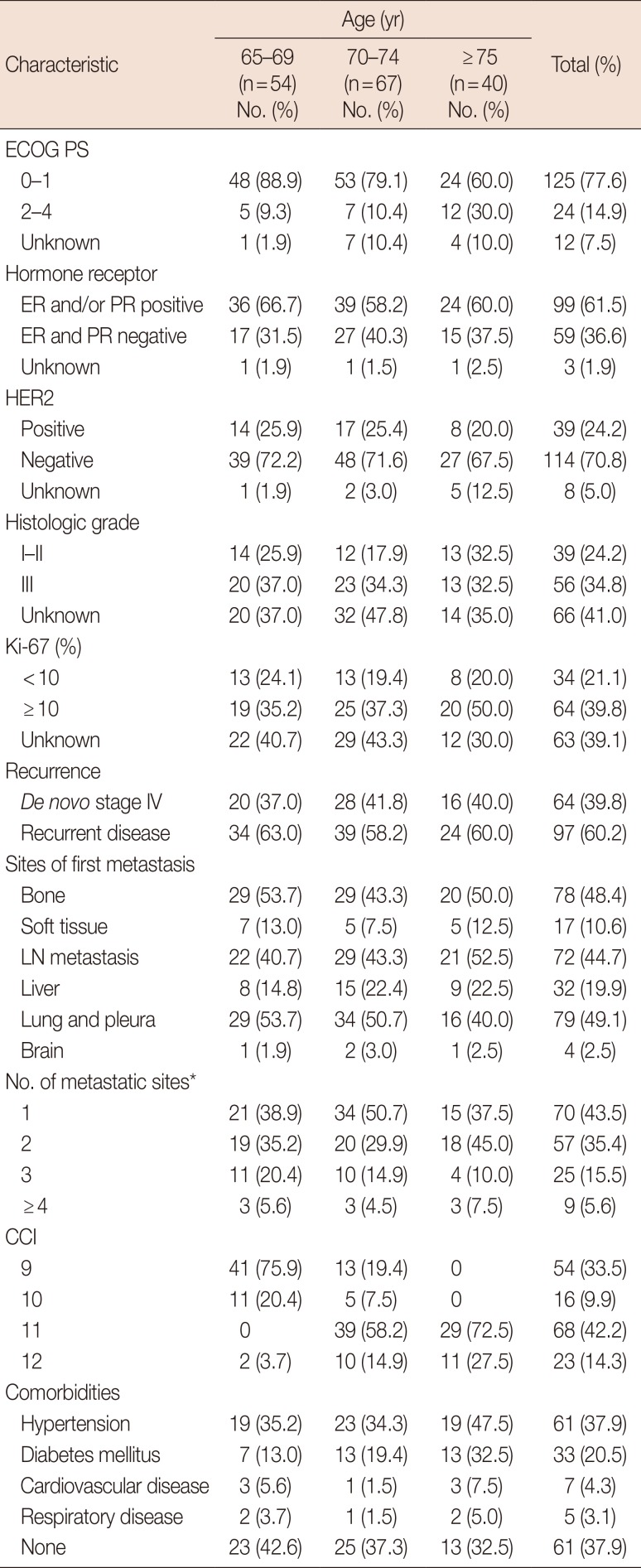
Table 1
Patient characteristics (n=161)
![]()
Treatment patterns
Treatment modalities according to age group are shown in Table 2. Hormonal therapy was the treatment of choice in patients aged ≥75 years, whereas chemotherapy was more frequently prescribed for patients aged <75 years. A total of 123 patients received at least one chemotherapy regimen, while 42.5% of patients aged ≥75 years did not receive any chemotherapy, compared to 17.9% of those aged 70 to 74 years and 16.7% of those aged 65 to 69 years (p=0.005), who did not receive any chemotherapy.
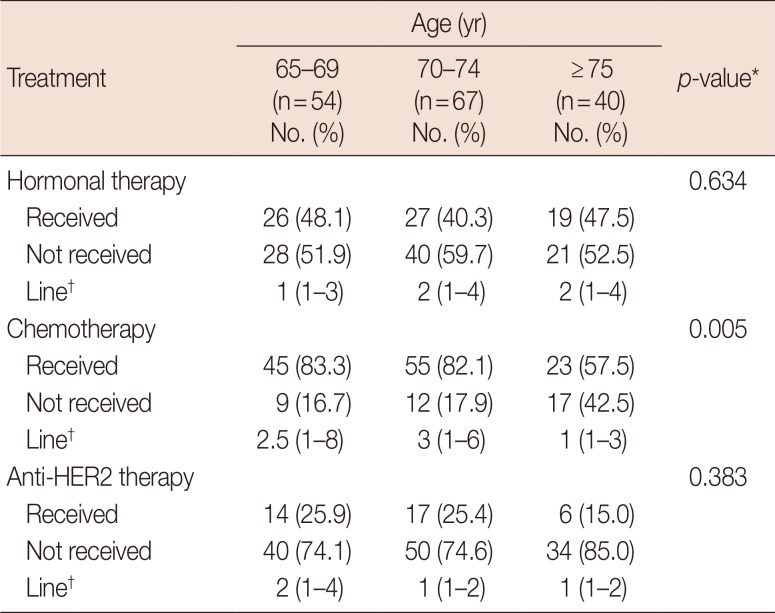
Table 2
Treatment modalities according to age group (n=161)
![]()
Hormonal therapy was indicated in a total of 72 patients, and a variety of agents were administered as palliative treatment for metastatic disease; 60 patients received nonsteroidal aromatase inhibitors (e.g., anastrozole and letrozole), while 40 patients received steroidal aromatase inhibitors (e.g., exemestane), 23 patients, tamoxifen, and 12 patients, fulvestrant. In recent 5 years, the U.S. Food and Drug Administration FDA-approved targeted agents such as everolimus and palbociclib were prescribed to four patients.
Among 39 HER2-positive patients, 48.7% presented with HR-positive tumors, while 94.9% (37/39) received at least one anti-HER2 therapy including trastuzumab, lapatinib, pertuzumab, and trastuzumab emtansine (T-DM1) in their treatment course. As first-line treatment, 31 patients received trastuzumab-based therapy; 28 patients received chemotherapy (27 received taxanes and one received gemcitabine) plus trastuzumab; two patients who were in the ≥75 years group received hormonal therapy plus trastuzumab; the remaining one patient received trastuzumab and taxanes with pertuzumab as first-line treatment. Subsequently, lapatinib was ad-ministered with capecitabine in a total of 16 patients, either as second-line or later-line treatment. The T-DM1 monotherapy was administered in five patients as third-line or later-line treatment. In the ≥75 years group, two patients did not receive any anti-HER2 therapy; one patient received hormonal therapy, and the other remaining patient received best supportive care only.
When we assessed the line of systemic treatment that patients received according to age group, all but one patient in the ≥75 years group received third-line treatment or were under-treated, while 45.6% of patients in the groups aged 70 to 74 years and 65 to 69 years received fourth-line or later-line treatment.
Nine patients received only best supportive care without additional treatment. Among these, five patients were in the ≥75 years group, three in the 70 to 74 years group, and one patient was in the 65 to 69 years group. Eight patients had ECOG PS ≥2 and six patients presented with a CCI score of ≥11. Seven patients presented with two or more metastatic sites, and all nine patients had visceral metastatic disease.
Factors affecting the selection of first-line treatment among HR-positive patients
Among 99 HR-positive patients, 49 and 44 patients received hormonal therapy and chemotherapy, respectively, as first-line treatment. The remaining six patients did not receive any systemic treatment; two patients received local treatment, and four patients received best supportive care only. Patient char-acteristics in the two treatment groups are listed in Table 3. Age distribution, HER2 status, and CCI scores were significantly different between the two groups (p=0.001, p=0.008, and p=0.010, respectively). In the multivariate logistic regression analysis, odds ratios (ORs) for receiving chemotherapy in the group aged 70 to 74 years and in those aged ≥75 years, in comparison to the group aged 65 to 69 years were 0.358 (p=0.228) and 0.010 (p=0.006), respectively. The ORs for receiving chemotherapy in HER2-positive patients compared to HER2-negative patients was 9.392 (p=0.014). The ORs for PS (2–4 vs. 0–1), metastatic sites (visceral vs. bone, soft tissue, and lymph node), and CCI (≥11 vs. 9–10) were 0.258 (p=0.189), 1.494 (p=0.484), and 1.852 (p=0.488), respectively. Thus, age ≥75 years and a HER2-negative status were significantly correlated with non-receipt of chemotherapy.
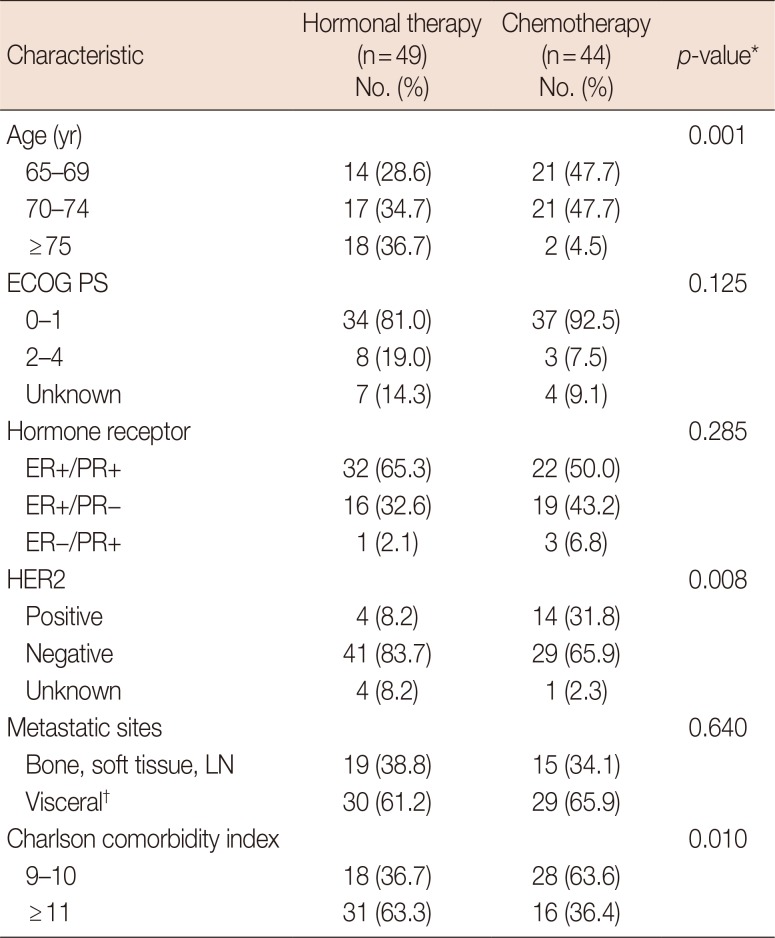
Table 3
Patient characteristics and first-line treatment modality among patients with hormone receptor-positive breast cancer
![]()
Chemotherapy as first-line treatment
We evaluated the feasibility of chemotherapy in 99 patients who received chemotherapy as first-line treatment by investigating type of chemotherapy, number of treatment cycles, and dose modifications of each chemotherapy regimen (Table 4). When chemotherapy was indicated for first-line treatment, 31 of 99 patients (31.3%) received combination chemotherapy and of these, 41.9% of patients received taxane-based regimens and 35.5% received anthracycline-based regimens. Thirty-nine of 99 patients (39.4%) received monochemotherapy; paclitaxel was prescribed in more than half of the patients (56.4%) followed by capecitabine (23.1%) and docetaxel (17.9%). When anti-HER2 therapy was indicated for HER2-positive patients (29.3%, 29/99), trastuzumab plus taxane was used as first-line chemotherapy in all but one patient, who received lapatinib plus capecitabine. Excluding anti-HER therapy, patients aged ≥75 years were more likely to receive mono-chemotherapy rather than combination chemotherapy (≥75 years, 83.3% vs. 16.7%; <75 years, 50.0% vs. 50.0%; p=0.034). Chemotherapy dose modifications were frequent regardless of the type of chemotherapy, and doses were mainly adjusted on the basis of the occurrence of adverse events in a prior course and the discretion of the treating physician. Dose reductions were more common in patients aged ≥75 years than in those aged <75 years (81.2% vs. 54.2%, not significant). The causes of early discontinuation of chemotherapy without progressive disease were as follows: chemotherapy-free interval after achievement of partial response or stable disease (24.2%, 24/99), adverse events (11.1%, 11/99), patient refusal (2.0%, 2/99), loss to follow-up (5.1%, 5/99), and unknown (2.0%, 2/99). Among HER2-positive patients, no cardiac adverse events such as left ventricular dysfunction (LVD) or heart failure related to anti-HER2 therapy were observed.
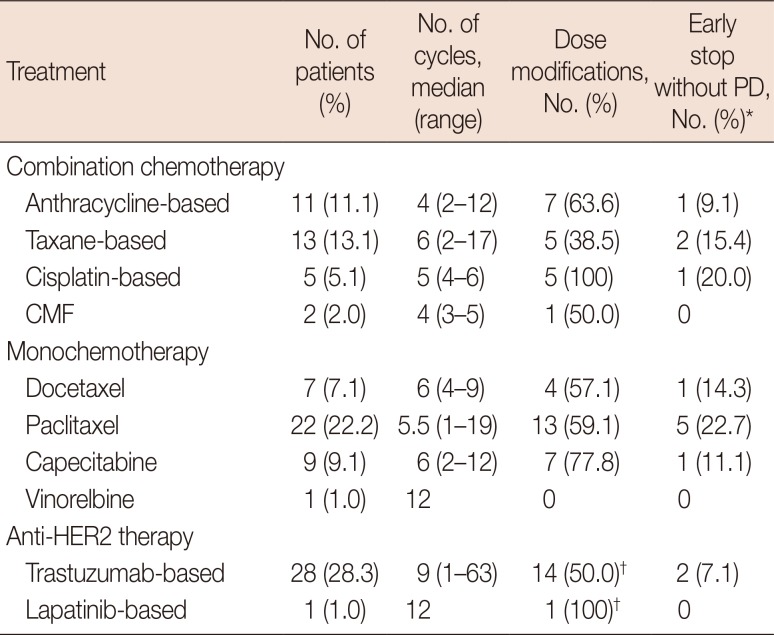
Table 4
Chemotherapy as first-line treatment in elderly patients with metastatic breast cancer (n=99)
![]()
Survival outcomes
At the time of this analysis (February 2017), 117 of 161 patients had died. The median OS for all patients was 30.3 months (95% confidence interval [CI], 23.3–36.6) across the entire patient population. The 1-year survival rate was 81.1% ±3.1% and 2-year survival rate was 56.7%±4.0% (Figure 1A). We also performed subgroup analyses for OS according to HR and HER2 status. The median OS of patients with HR-positive/HER2-negative (n=74), HER2-positive (n=39), and triple-negative tumors (n=39), was 35.0 months (95% CI, 23.3–46.7), 32.7 months (95% CI, 13.2–52.2), and 17.7 months (95% CI, 12.8–22.6), respectively (Figure 1B). When we assessed OS according to type of systemic treatment that patients received, all types of systemic treatments were found to significantly improve patient survival. A total of 123 patients received at least one chemotherapy regimen during their treatment course, and the median OS for these patients was 32.7 months (95% CI, 22.2–43.1), in comparison to 15.2 months (95% CI, 12.7–17.6) in patients who did not receive any type of chemotherapy (p=0.004) (Figure 2A). Among 39 triple-negative patients, for whom chemotherapy was the treatment of choice, the median OS of 35 patients who received at least one chemotherapy regimen was 18.7 months (95% CI, 15.2–22.2), while that of four patients who did not, was only 2 months (95% CI, 0.5–3.5). In a total of 99 HR-positive patients for whom hormonal therapy was indicated, the median OS of 72 patients who received at least one hormonal therapy and that of 27 patients who did not was 47.4 months (95% CI, 31.1–63.6) and 18.8 months (95% CI, 7.1–30.5), respectively (p=0.002) (Figure 2B). Lastly, of the total of 39 HER2-positive patients, the median OS of 37 patients who received at least one anti-HER2 therapy was 35.4 months (95% CI, 15.8–54.9), while that of two patients who did not, was 14.3 months (p=0.004) (Figure 2C). In contrast to the above data, the median OS of 13 patients (four who received local treatment and nine who received best supportive care) who did not receive any type of systemic treatment was only 5.2 months (95% CI, 2.9–7.4).
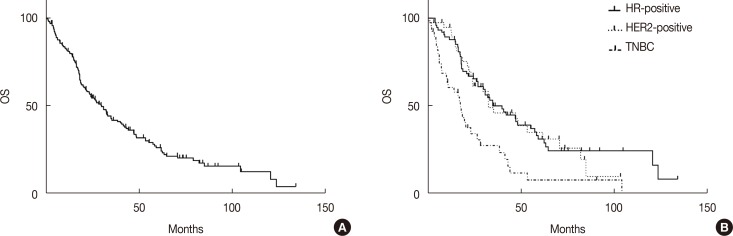 | Figure 1The Kaplan-Meier survival curves for overall survival (OS). Survival curves for OS in all patients (n=161) (A). Survival curves for OS according to biologic subtype (B).HR=hormone receptor; HER2=human epidermal growth factor receptor 2; TNBC=triple-negative breast cancer.
|
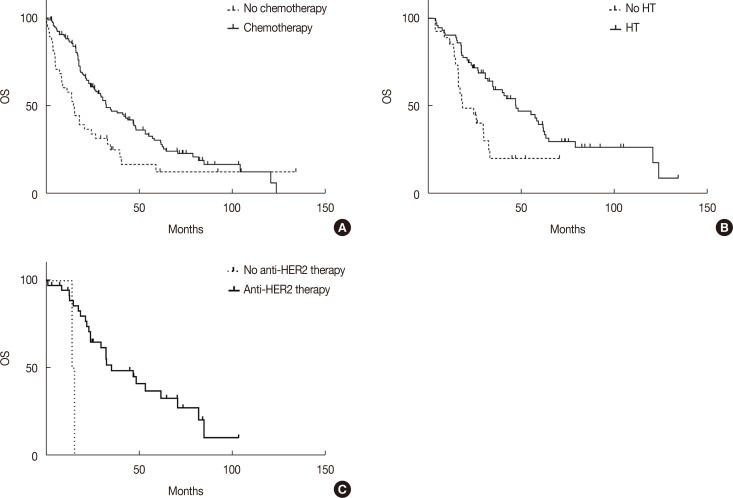 | Figure 2The Kaplan-Meier survival curves for overall survival (OS) according to treatments. Survival curves for OS in patients who received at least one chemotherapy regimen compared to those who did not (A). Survival curves for OS in patients who received at least one hormonal therapy compared to those who did not (B). Survival curves for OS in patients who received at least one anti-HER2 therapy compared to those who did not (C).HT=hormonal therapy; HER2=human epidermal growth factor receptor 2.
|
When we analyzed the prognostic factors affecting OS, we found that age, ECOG PS, combined HR and HER2 status (triple-negative status), and number of metastatic sites were significantly associated with OS, and were significant in both univariate and multivariate analyses (Table 5). The unadjusted median OS of patients aged 65 to 69 years was significantly longer than those of patients in the other age groups (65–69 years, 47.1 months [95% CI, 40.1–54.0]; 70–74 years, 28.4 months [95% CI, 20.5–36.2]; ≥75 years, 18.1 months [95% CI, 14.2–21.9]; p=0.001); the hazard ratios in the groups aged 70 to 74 years and ≥75 years, in comparison to the group aged 65 to 69 years were 1.855 (95% CI, 1.143–3.011) (p=0.011) and 2.111 (95% CI, 1.237–3.603) (p=0.006), respectively, in multivariate analyses. Furthermore, we also performed prognostic factor analyses for OS only in patients 70 years and older, while excluding patients aged 65 to 69 years. The ECOG PS, triple-negative cancer, and number of metastatic sites were significant poor prognostic factors for OS in the multivariate analyses, while age was not a significant factor for OS in this age group (data not shown).
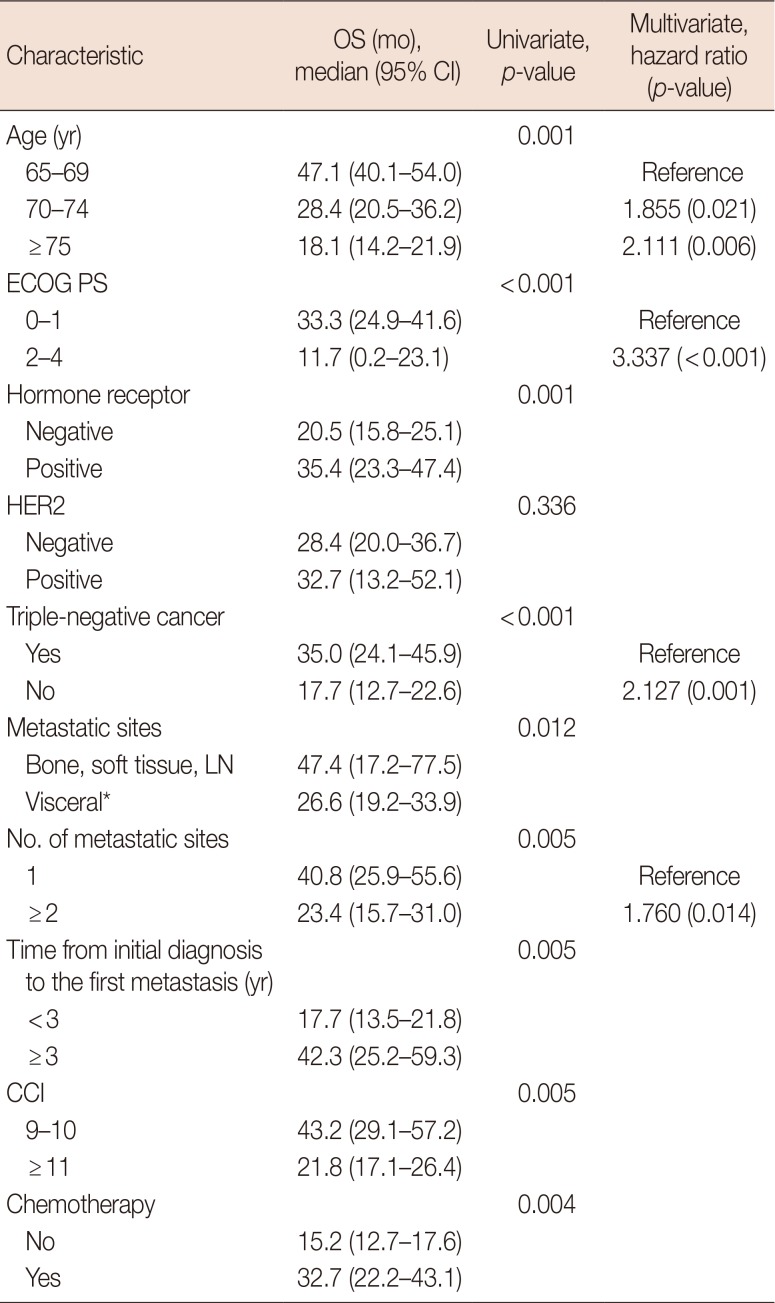
Table 5
Prognostic factor analyses for overall survival (n=161)
![]()
Go to :
DISCUSSION
The objective of this retrospective study was to investigate demographic and clinicopathologic characteristics, treatment patterns, and follow-up treatment outcomes in patients with MBC aged 65 years and older. In this study, patients ≥75 years were more likely to have a poor ECOG PS (≥2) and advanced comorbidity (CCI ≥11), compared to those in the other age groups. In a study of MBC patients aged 65 years and older in France, Freyer et al. [15] also reported that elderly patients were more likely to present with initial metastasis (>75 years, 52%; 65–74 years, 39%; p<0.0001), and the incidence of an ECOG PS of 0 in patients aged 64 to 75 years was more frequent than in those aged >75 years (25% vs. 9%, p<0.0001).
Regarding decisions about systemic treatment for MBC in elderly patients, biologic subtype guides treatment, as in younger patients. Hormonal therapy is the approach of choice for HR-positive metastatic disease. Anti-HER2 therapy should be used or added to the endocrine or chemotherapy regimen when the cancer is HER2-positive. For MBC that is HR-negative, has been refractory to hormonal therapy, or is rapidly progressing disease, chemotherapy is indicated [16]. When we investigated treatment patterns according to age group in this study, patients aged ≥75 years were less likely to receive chemotherapy compared to those aged <75 years; however, there were no significant differences pertaining to the receipt of hormonal therapy and anti-HER2 therapy. In addition, age was one of the most important deciding factors in the selection of chemotherapy (versus hormonal therapy) as first-line treatment among HR-positive patients; the OR for receiving chemotherapy in the group ≥75 years in comparison to the group aged 65 to 69 years was 0.010 (p=0.006). Age has already been reported to be a significant factor related to treatment selection in elderly patients with MBC [1517].
When chemotherapy was indicated for first-line treatment, taxanes were the most commonly prescribed chemotherapy agents, regardless of HER2 status. Dose modifications were common irrespective of the types of chemotherapy, and early discontinuation of chemotherapy due to adverse events or patient refusal was observed in 13.1% of patients. In a study of 7-year retrospective analysis of 117 MBC patients aged ≥75 years receiving first-line chemotherapy, 103 received monotherapy (67, capecitabine; 29, vinorelbine; five, docetaxel; two, liposomal doxorubicin) and 14 received polychemotherapy (12, anthracycline-based; two, vinorelbine-gemcitabine), with acceptable toxicity [18]. Data on chemotherapy for elderly patients with MBC remain very limited, while adjuvant chemotherapy has been reported to be feasible in most patients aged ≥70 years who are selected for chemotherapy, although increasing age, lower functional status, and higher comorbidity index scores have been associated with dose reductions and treatment breaks in chemotherapy [1920]. The International Society of Geriatric Oncology recommends that in elderly patients with MBC, single-agent chemotherapy should be generally preferred to combination regimens, and preference should be given to chemotherapeutic agents that have better safety profiles (such as weekly taxanes, pegylated liposomal doxorubicin, capecitabine, and vinorelbine), and those with safety data available in elderly patients [162122232425]. Recently, prediction models for chemotherapy toxicity, which estimated risk of toxicity based on clinical factors in addition to geriatric assessment variables, have been developed and can be used to help weigh the risks and benefits of chemotherapy [1314]. These models, however, require further validation in specific diseases and with particular treatments.
In this study, anti-HER2 therapy was indicated in 39 HER2-positive patients. There was no significant difference in the receipt of anti-HER2 therapy based on age; in fact, all but two patients received at least one anti-HER2 therapy in their treatment course. Data are limited regarding treatment patterns and outcomes in elderly patients with metastatic HER2-positive breast cancer. In the registHER observational study of 1,001 women (209 women aged ≥65 years) with newly diagnosed metastatic HER2-positive breast cancer, patients aged ≥75 years were least likely to receive trastuzumab-based first-line treatment (≥75 years, 77% [50/65]; 65–74 years, 81% [117/144]; <65 years, 85% [674/792]). In addition, among all patients receiving trastuzumab-based first-line treatment, pa-tients aged ≥75 years were more likely to receive either trastuzumab monotherapy or trastuzumab with hormonal therapy, rather than trastuzumab-based chemotherapy regimens [26]. In our study, among the 28 patients who received trastuzumab with chemotherapy as first-line treatment, most patients continued to receive trastuzumab until progression even if chemotherapy was discontinued after disease stabilization. In terms of cardiac toxicity, no LVD or heart failure were observed in our study, although recent population-based studies have shown that the incidence of heart failure or cardiomyopathy may be high in elderly patients [2728].
When we analyzed survival outcomes, the median OS for all patients was 30.3 months (95% CI, 23.3–36.6) across the entire patient population. The OS according to biologic subtype were as follows: 35.0 months (95% CI, 23.3–46.7) in HR-positive/HER2-negative patients, 32.7 months (95% CI, 13.2–52.2) in HER2-positive patients, and 17.7 months (95% CI, 12.8–22.6) in patients with triple-negative status. As previously described, our study has also shown that anti-HER2 therapy is associated with a significant improvement in OS of elderly patients with HER2-positive MBC. In the registHER study, when data were analyzed on the basis of receipt of first-line trastuzumab or not, OS was significantly longer for older women receiving trastuzumab compared to those who did not (median OS, 40.4 months vs. 25.9 months) [26]. In another study of a large cohort (n=610) of elderly patients (mean age, 74 years) with HER2-positive MBC, Griffiths et al. [29] reported that trastuzumab plus chemotherapy was associated with a lower adjusted cancer mortality rate (hazard ratio, 0.54; 95% CI, 0.39–0.74; p<0.001) than trastuzumab alone among patients who received trastuzumab as part of first-line therapy. In our study, we observed that the HER2 testing was less frequently performed among patients ≥75 years than those aged 65 to 74 years. Since anti-HER2 therapy improved survival outcome in HER2-positive MBC across age groups, we believe that the HER2 testing should be routinely performed for all elderly patients. Among 39 triple-negative patients in our study, for whom chemotherapy was the approach of choice, the median OS of 35 patients who received at least one chemotherapy regimen was 18.7 months (95% CI, 15.2–22.2), while that of four patients who did not, was only 2.0 months (95% CI, 0.5–3.5). In one population-based study of elderly patients aged ≥66 years and with metastatic ER-negative breast cancer, chemotherapy was associated with a significant survival benefit (hazard ratio, 0.61; 95% CI, 0.54–0.70) [30]. In real-world clinical practice, elderly cancer patients are less likely to be offered chemotherapy and tend to receive less intensive treatment because of concerns regarding their ability to tolerate the therapy. However, in this study, we found that chemotherapy was feasible as first-line treatment, and significantly improved patient survival in the elderly. However, patients aged ≥75 years were more likely to have a poor ECOG PS and advanced comorbidity, and tended to receive no chemotherapy or less intensive chemotherapy. Freyer et al. [15] also reported that age was found to be a strongly discriminating factor in treatment decisions: a cutoff threshold for differential treatment based on age was 76.5 years.
Multivariate analyses for OS performed across the entire patient population, showed that age (≥70 years), poor PS (ECOG 2–4), triple negative cancer, and number of metastatic sites (≥2) were significant poor prognostic factors for OS. Among patients aged ≥70 years, poor PS (ECOG 2–4), triple-negative cancer, and number of metastatic sites (≥2) were also significant poor prognostic factors for OS in multivariate analyses.
This retrospective study has several limitations. We could not identify accurately the reasons as to why patients aged ≥75 years had received less intensive treatment: if due to patient choice or due to the physician discretion. We also could not determine the geriatric assessment variables that may be associated with increased risk of treatment toxicity and survival outcomes, since they were not evaluated in routine clinical practice. In addition, the safety and efficacy of chemotherapy could not be assessed by retrospective chart review, as accurately as in prospective clinical trials.
In conclusion, the majority of patients received active treatment according to the biologic cancer subtype as in younger patients, although frequent dose modifications were observed during chemotherapy. All types of systemic treatment conferred more prolonged OS, although many patients who did not receive systemic treatment had poor prognostic factors such as poor PS and advanced comorbidity. In this regard, we therefore recognize the fact that elderly patients with MBC who are considered fit for systemic treatment should not be excluded from receiving active treatment with the appropriate regimens and dose intensity. In addition, future research plans for elderly patients, especially those aged ≥75 years with breast cancer, should include a geriatric assessment that could be utilized to identify patients at risk for treatment-related toxicity, and also to select patients who could benefit from active treatment. Overall, this analysis of elderly patients with MBC will provide a better understanding of this population and help guide clinical care in real-world practice.
Go to :
 XML Download
XML Download