

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Parkinson's disease (PD) is the second most common neurodegenerative disease. Idiopathic PD accounts for approximately 90% of all cases of PD [1], and several factors including coffee and tea consumption, smoking, drinking well water, and pesticide exposure have been reported to affect the risk of idiopathic PD [2]. According to worldwide epidemiological data, men exhibit a higher risk of PD than do women, and estrogen is suggested to play a neuroprotective role in this difference in risk [34]. Furthermore, high lifetime estrogen exposure and estrogen-based replacement therapy in postmenopausal women have been reported to be associated with a reduced risk of PD [56].
Tamoxifen, an estrogen modulator, is widely used in the treatment of estrogen receptor-positive breast cancer because of its estrogen antagonist effect. A study performed using the Danish Breast Cancer Collaborative Group database showed an increased risk of PD 4 to 6 years after initiation of tamoxifen treatment [7]. However, tamoxifen demonstrated neuroprotective effects in several in vitro and in vivo studies [89]. Because tamoxifen is the treatment of choice for estrogen receptor-positive breast cancer and its effect on neurons is unclear, further investigation to determine whether tamoxifen alters the risk of PD is required.
Go to : 
METHODS
Study design and cohort
The present study has a retrospective population-based cohort design. The study cohort consisted of one group of female patients with breast cancer who received tamoxifen treatment and one group comprising patients with breast cancer who were not exposed to tamoxifen. The patients were selected from 2 million beneficiaries of Taiwan's National Health Insurance program, randomly sampled from Taiwan's entire population of 23 million. All information was obtained from Taiwan's National Health Insurance Research Database (NHIRD), which has been described previously [1011]. The NHIRD includes information on disease diagnoses classified according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) codes, treatment procedures, dates of service, prescribed medications that can be classified according to the Anatomical Therapeutic Chemical (ATC) system of medications, reimbursement amounts, patient demographic characteristics, and encrypted patient and provider identifiers. Data were collected from 2000 to 2009. This study was approved by the Joint Institutional Review Board of Taipei Medical University (approval number: N201509045) and performed in accordance with the principles of the Declaration of Helsinki. In this retrospective outcomes study, the informed consent was waived.
Study patients
The patients with breast cancer were identified from among those included in the NHIRD between 2000 and 2009 on the basis of the diagnosis code (ICD-9-CM code: 174, malignant neoplasm of female breast). Patients with a diagnosis of skin neoplasm of the breast (ICD-9-CM codes: 172.5 and 173.5) were excluded. The duration of tamoxifen (ATC code L02 BA01) treatment was identified according to prescriptions.
The main outcome measure was the development of PD, identified by the presence of the PD diagnosis code (ICD-9-CM code: 332.0), with a history of prescription of dopaminergic medicine (ATC code N04B) and without any history of cerebrovascular accident (ICD-9-CM code: 430–438) 1-year before the diagnosis of PD. Secondary parkinsonism (ICD-9-CM code: 332.1) was excluded. According to Lee et al. [12], the diagnostic criteria had been validated with an accuracy of 94.8%.
Statistical analysis
The patients in both groups were followed from the index diagnosis date until December 31, 2009. The follow-up period ranged from 1 to 10 years. The standardized differences among all covariates were used to evaluate the differences between female patients who did and did not receive tamoxifen treatment. Logistic regression was used to calculate propensity scores. Cox proportional hazards regression analysis was performed to compare the risk of PD between the patients who did and did not receive tamoxifen treatment. Diabetes and gout were included in the model as adjustment factors due to previous evidence regarding associations between these diseases and PD [131415]. In addition, prescription of any of the aforementioned drugs with neuroprotective potential was included in the adjustment. All analyses were performed using SAS/STAT 9.2 software (SAS Institute Inc., Cary, USA) and STATA 12 software (StataCorp LP, College Station, USA). A p-value of 0.05 was considered significant.
Go to :
RESULTS
Our study included 5,185 and 5,592 patients with breast cancer who did and did not receive tamoxifen treatment, respectively, and all the patients were women. The mean follow-up periods were 62.77±38.89 and 59.13±40.52 months in the groups of patients who did and did not receive tamoxifen treatment, respectively. In the 5,185 patients with breast cancer and a history of tamoxifen treatment, the average treatment duration was 29.97±23.97 months. No significant differences were observed between the groups in history of diabetes, gout, or prescription of lipophilic statins (Table 1). The percentage of patients with a history of hypertension, pre-scription of dihydropyridine derivative calcium channel blockers (CCBs), metformin, or pioglitazone was significantly higher in the group of patients who received tamoxifen treatment. Furthermore, the average age for the group that received tamoxifen treatment was significantly higher than that for the group that did not receive tamoxifen treatment (52.4±12.1 and 50.9±12.8 years, p<0.001). Overall, the tamoxifen-treated group manifested more comorbidity, which was calculated using the Charlson comorbidity index (CCI) [16].
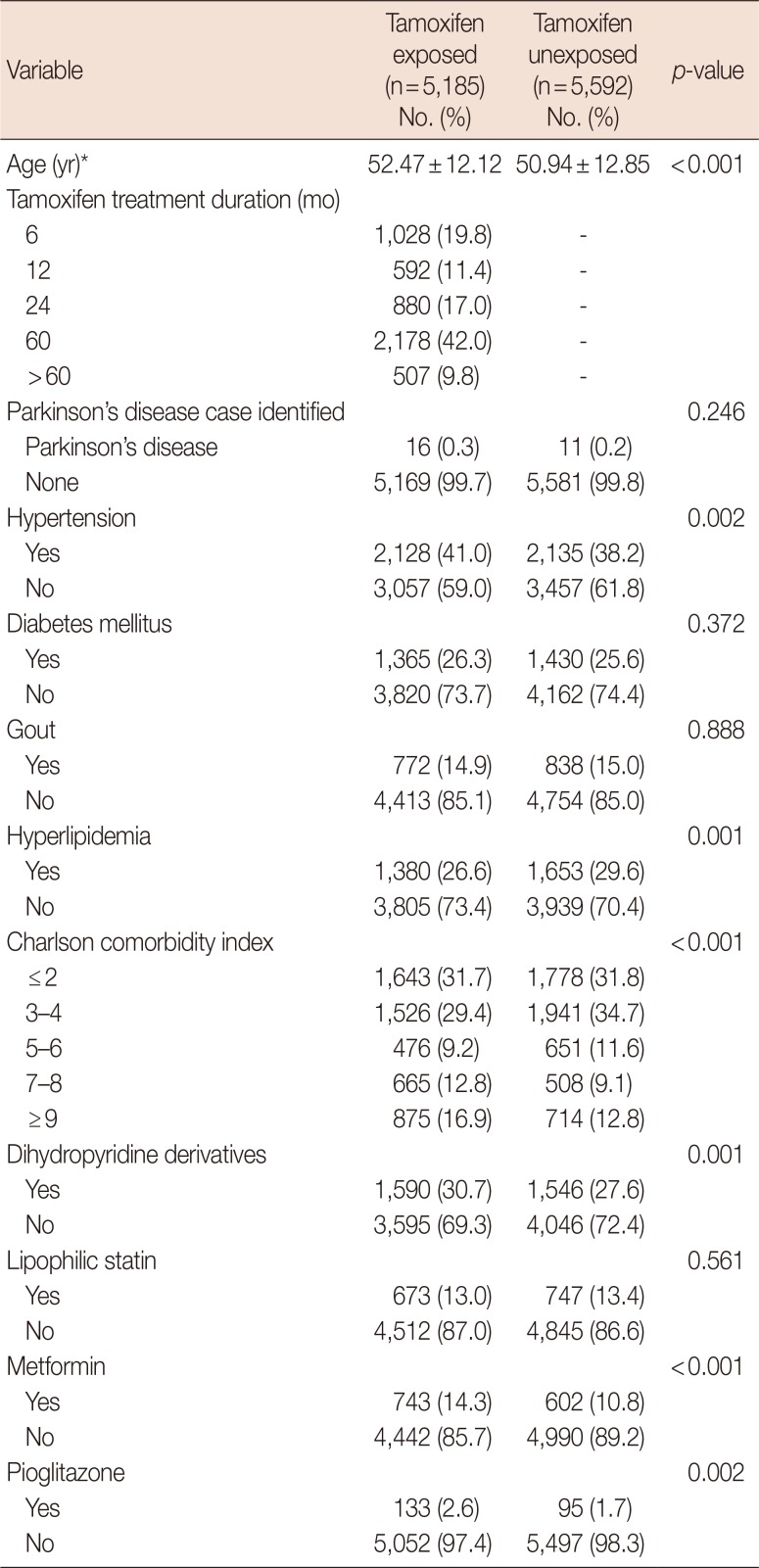
Table 1
Demographic data for tamoxifen exposed and unexposed groups
![]()
During the follow-up period (2000–2009), 16 (0.3%) and 11 (0.2%) patients who did and did not receive tamoxifen treatment, respectively, developed PD. No significant increase in the crude hazard ratio (HR) of developing of PD was observed in tamoxifen-treated women (HR, 1.56; 95% confidence interval [CI], 0.73–3.39; p=0.246). After adjustment for age, hypertension, diabetes, gout, hyperlipidemia, CCI, prescription of dihydropyridine derivative CCBs, lipophilic statins, metformin, and pioglitazone, the adjusted HR (aHR) of developing PD was 1.310 (95% CI, 0.605–2.837; p=0.494) for the group that received tamoxifen treatment compared with the group that did not receive tamoxifen treatment (Table 2). Further analysis of the risk of developing PD with different treatment durations revealed a significant increase in the risk of PD among patients who underwent follow-up for more than 6 years (aHR, 2.435; 95% CI, 1.008–5.882; p=0.048) (Table 3).

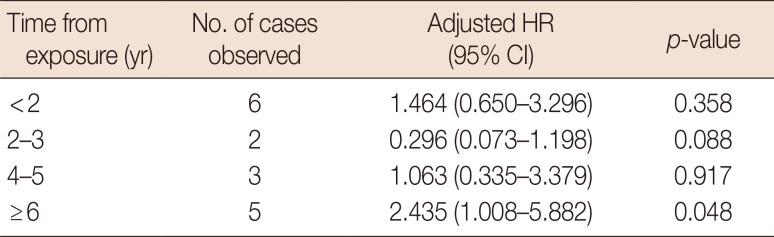
Table 2
The adjusted HR of Parkinson's disease for tamoxifen treatment group*
| Tamoxifen | Regression coefficient | Adjusted HR (95% CI) | p-value |
|---|---|---|---|
| Unexposed | 0 | 1 | |
| Exposed | 0.270 | 1.310 (0.605–2.837) | 0.494 |
![]()
Table 3
The adjusted HR of Parkinson's disease for tamoxifen treatment group in different treatment duration
![]()
Go to :
DISCUSSION
The results of the present study, similar to the findings of previous research, demonstrated that tamoxifen treatment increased the risk of PD in Taiwanese female patients with breast cancer in long-term follow-up. This evidence may raise the level of concern about the neurotoxic effects of tamoxifen, which is the first-line treatment for estrogen receptor-positive breast cancer in women.
It remains controversial whether tamoxifen has neuroprotective or neurotoxic effects on the dopaminergic system. In animal studies, tamoxifen prevents the loss of dopaminergic neurons caused by methamphetamine-induced toxicity in male mice in a dose-dependent manner [17]. In addition, tamoxifen prevents methamphetamine-induced parkinson-ian-like features in female mice [18]. However, Gao and Dluzen [19] reported the negative impact of tamoxifen. Their findings showed that tamoxifen abolished the neuroprotective effect of estrogen on methamphetamine neurotoxicity in the dopaminergic system.
The present study analyzed a nationwide population database and demonstrated that tamoxifen increases the risk of PD in Taiwanese female patients with breast cancer in the long term (>6 years follow-up). The results of the present study were similar to those of a Danish study that showed an increased risk of PD 4 to 6 years after initiation of tamoxifen treatment [7]. In Caucasians, individuals of male sex are at higher risk of PD [2021]. Based on this gender difference, estrogen is speculated to be neuroprotective, which accounts for the increased PD risk associated with tamoxifen. While there is no such gender difference in Taiwan [2223], we nonetheless observed the possible neurotoxicity of tamoxifen. This conflict raises two more questions: is estrogen really neuroprotective, and is there any extra-estrogen effect of tamoxifen that could trigger the increased risk of PD? In fact, the protective ability of estrogen in relation to PD is still debatable. A review by Liu and Dluzen [24] included 14 studies investigating the effect of estrogen in patients with PD: seven showed a neuroprotective effect of estrogen, whereas four showed anti-dopaminergic effects, and three showed no effect. Meanwhile, tamoxifen may induce cytotoxic autophagy [25] and mitochondrial dysfunction [26], which may trigger neurodegeneration.
The present study exhibits certain limitations. The NHIRD does not provide information on some lifestyle-related risk factors, such as smoking, coffee consumption, drinking well water, and pesticide exposure. Smoking is a crucial risk factor because it is highly associated with both breast cancer and PD; the rate of female smokers in Taiwan is much lower than that in Western countries and the smoking habit is initiated at a later age [27]. Additionally, the misclassification of PD in the NHIRD is a concern. Although validation has previously been performed by medical chart review, the gold standard for PD diagnosis is based on clinical investigation and neurological examination by neurologists. Furthermore, the NHIRD does not provide the subtype of the diagnosed breast cancer. Tamoxifen is the treatment of choice for patients with estrogen receptor- or progesterone receptor-positive breast cancer, who were shown in a previous study to exhibit better 5-year survival and overall disease survival than patients with estrogen receptor- or progesterone receptor-negative breast cancer [2829]. However, in the present study, the mean follow-up period was not significantly different between the patients who did and did not receive tamoxifen treatment, which indicated that the incidence of PD did not affect survival. Furthermore, the different receptor status of breast cancer affects not only the choice of tamoxifen treatment, but also the requirement for chemotherapy and the treatment regimen [30]. Since chemotherapy is strongly associated with tamoxifen treatment, it would be difficult to exclude the effect of chemotherapy on the risk of PD in the present study.
In summary, tamoxifen was associated with an increased risk of PD after more than 6 years of follow-up. This result may raise further concerns regarding the safety of administering tamoxifen for Asian female patients with estrogen receptor-positive breast cancer. A global and multiracial survey will be required in the future to completely elucidate the association between tamoxifen treatment and the risk of PD.
Go to :
 XML Download
XML Download