

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the most frequently diagnosed cancer worldwide and the leading cause of cancer death in women, accounting for 25% of all female cancers and 14% of all cancer-related deaths [1]. In general, 20% of patients with early breast cancer experience recurrence or distant metastasis within 5 years after the initial diagnosis [2]. Although recent improvements in the treatment of metastatic breast cancer (MBC) have prolonged the median survival of MBC patients, no therapeutic options have been established for patients who failed standard treatment. As such, the treatment results of cyclophosphamide, methotrexate, and 5-fluorouracil (CMF) chemotherapy, which was widely used in the early years of chemotherapy, should be re-evaluated.
Majority of MBC patients are treated with anthracycline and taxane as a first-line therapeutic option. Capecitabine was approved in 1998 by the U.S. Food and Drug Administration as a single agent for MBC resistant to both paclitaxel and anthracyclines [34]. Eribulin mesylate was also indicated for MBC patients who have previously received at least two chemotherapeutic regimens [5]. For non-responsive patients, additional cytotoxic chemotherapy is usually administered and is used as third-line or later treatment as follows: vinca alkaloid [6], gemcitabine [7], ixabepilone [8], and albumin-bound paclitaxel [9]. All the above-mentioned agents showed modest activity and tolerable toxicity profiles. Many reports described an increased median survival for MBC patients, and this trend was related to the availability of several therapeutic agents [10111213]. Additionally, a meta-analysis regarding survival data from 128 randomized trials concluded that the gain in absolute survival from anthracyclines; taxanes; nontaxanes, such as capecitabine and gemcitabine; and trastuzumab, either as monotherapy or combined therapy, ranged from 4.2 to 12.5 months for a patient with an anticipated survival of 1 year compared with a treatment with the reference standard alone [13].
CMF chemotherapy has been among the traditional adjuvant chemotherapy options for early stage breast cancer. Studies about the use of CMF therapy have shown that its use as an adjuvant treatment improves disease-free survival (DFS) and overall survival (OS) [1415]. The combination of doxorubicin and cyclophosphamide chemotherapy (four cycles) increases relapse-free survival and OS, equivalent to that obtained after CMF chemotherapy [1416]. Moreover, in the results from the Early Breast Cancer Trialists' Collaborative Group, an overview analysis regarding adjuvant polychemotherapy has shown that anthracycline-containing regimens reduce recurrence and prolongs survival compared with CMF [17]. Additionally, adjuvant taxanes significantly improved the rates of DFS and OS among women with node-positive breast cancer [18]. Recently, docetaxel with cyclophosphamide showed OS benefit compared with doxorubicin and cyclophosphamide [19]. The shift to using anthracyclines and taxanes in the early stages of disease, including as adjuvant therapy, has increased the risk for recurrences of MBC patients after treatment with other agents.
Although new agents have been developed for the treatment of MBC, the Korean National Health Insurance does not cover all the new drugs, particularly those that are costly. In terms of cost-effectiveness, CMF is generally among the most cost-effective and feasible treatment options for MBC patients.
The pharmacokinetics of CMF as adjuvant therapy suggests that it can have a relevant role in the treatment of heavily pretreated patients. Our study aimed to determine a salvage treatment with CMF for anthracycline- and taxane-pretreated MBC.
Go to : 
METHODS
Study population
We consecutively enrolled 158 MBC patients who underwent CMF chemotherapy as palliative treatment at Seoul National University Hospital and Seoul Metropolitan Government-Seoul National University Boramae Medical Center between 2002 and 2016. For all eligible patients, the status of estrogen receptor (ER), progesterone receptor, and human epidermal growth factor receptor 2 (HER2) was evaluated via immunohistochemical staining or fluorescence in situ hybridization (only for HER2 characterization). The MBC was classified accordingly into hormone receptor (HR) positive (HR-positive/HER2-negative), HER2 positive (HR-positive or negative/HER2-positive), and triple-negative breast cancer (TNBC) (HR-negative/HER2-negative) according to the status of ER, progesterone receptor, and HER2. In 100 patients (63.3%), the treatment modality of choice was a regimen of oral cyclophosphamide (100 mg/m2 daily) from day 1 through day 14 in combination with methotrexate (40 mg/m2) and 5-fluorouracil (600 mg/m2) intravenous injection at day 1 and 8, administered every 4 weeks. In 58 patients (36.7%), a regimen of intravenous cyclophosphamide (600 mg/m2 intravenously) in combination with methotrexate (40 mg/m2) and 5-fluorouracil (600 mg/m2) was administered on day 1, every 3 weeks. The clinician decided on the patient's specific therapeutic regimen. Treatment was continued until disease progression (PD) or intolerable toxicity was observed or if the patient refused to continue treatment.
Clinical evaluation and response criteria
The response to treatment was evaluated by using computed tomography every three cycles of treatment or earlier when signs of PD according to the Response Evaluation Criteria in Solid Tumors (1.1) were evident. Patients who had complete response (CR) or partial response (PR) were defined as responders. The disease control rate (DCR) reflects the proportion of patients who had CR, PR, and stable disease (SD).
Statistical analyses
The categorical variables were statistically analyzed using Pearson chi-square test or Fisher exact test. The median durations of progression-free survival (PFS) and OS were calculated by using the Kaplan-Meier method. Comparisons between different groups were made by using the log-rank tests. Multivariate analyses were performed using a Cox regression model for PFS and OS to identify independent factors and adjust for baseline characteristics. Two-sided p-values of <0.05 were considered significant. All analyses were performed using SPSS for Windows version 20.0 (IBM Corp., Armonk, USA).
This study was approved by two academic hospitals in South Korea (IRB numbers: J-1612-114-816 and 26-2016-173). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Go to :
RESULTS
Patient characteristics
The baseline demographic and clinicopathologic information of the 158 patients enrolled in this study is summarized in Table 1. The median follow-up for all patients was 9.1 months (range, 0.8–93.0 months). At the time of this analysis (February 2017), 144 of the 158 patients had died. The median interval between MBC diagnosis and CMF treatment was 36.0 months (range, 7.1–146.7 months). The most frequently involved metastatic organ was the lung, followed by the bone, lymph nodes, and liver. The majority of patients had an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0–1.
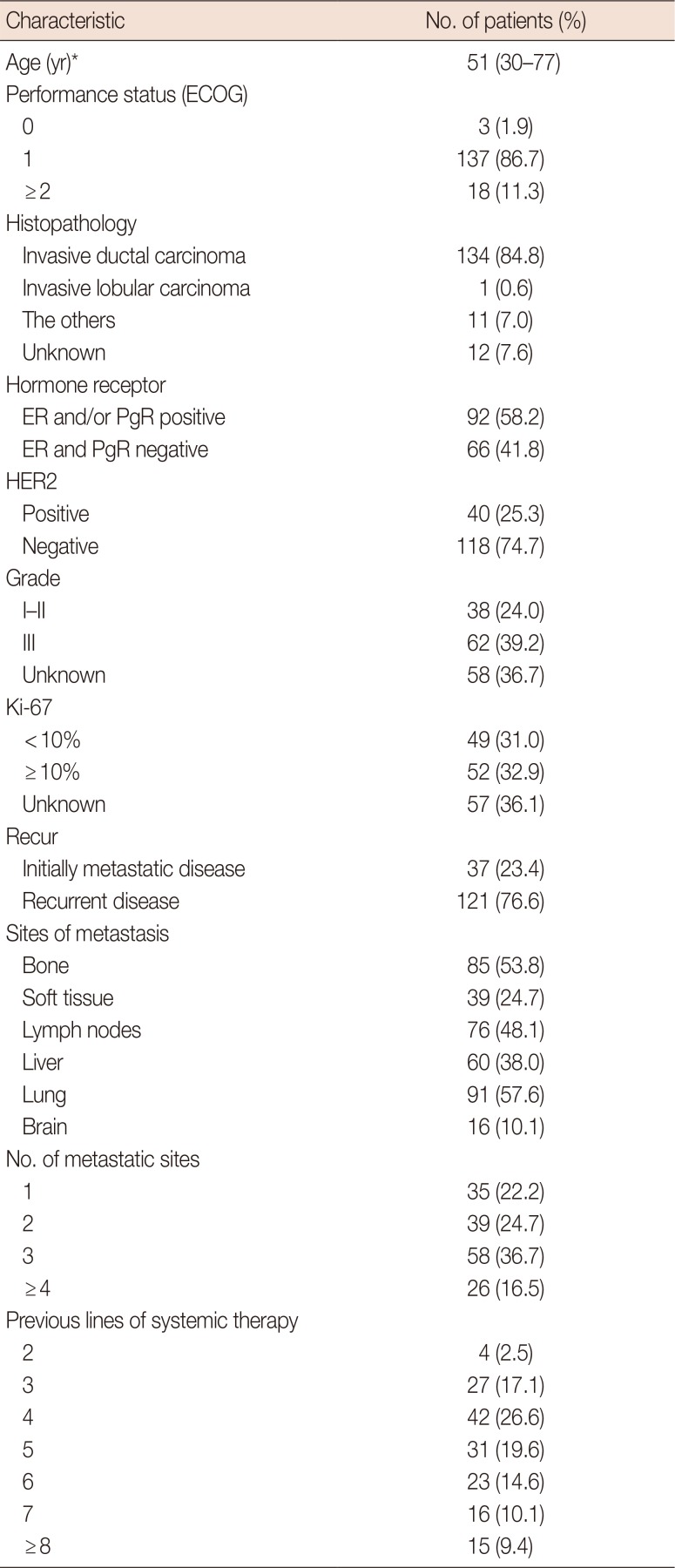
Table 1
Patient characteristics (n=158)
![]()
Based on the HR and HER2 status, 73 (46.2%), 40 (25.3%), and 45 (28.5%) tumors were classified as HR positive, HER2 positive, and TNBC, respectively. Among the patients with the HER2-positive subtype, 39 (97.5%) and 27 (67.5%) patients were treated with trastuzumab and lapatinib before CMF administration, respectively. Only one patient received trastuzumab along with CMF. In 92 HR-positive patients, 74 (80.4%) received at least hormone therapy before CMF administration. All the patients except one (157, 99.4%) received previous taxane-based chemotherapy, and 154 (97.5%) received prior anthracycline-based chemotherapy. Regarding other therapeutic choices for the patients enrolled in the study, 149 (94.3%), 139 (88.0%), and 138 (87.3%) patients were treated with gemcitabine, capecitabine, and vinorelbine, respectively. Patients were heavily pretreated, as they had received a median of 5 prior regimens (range, 2–11 regimens), including a median of 1 prior hormone therapy (range, 0–5) in HR-positive patients.
Tumor response
Tumor response was evaluated in 147 patients (93.0%). In the remaining patients, the response could not be assessed due to loss to follow-up, transfer to another hospital, and death. As the best response, we observed CR in one, PR in 15, SD in 49, and PD in 82 patients. Therefore, the overall response rate (CR+PR) to CMF treatment was 10.9%, and the DCR was 44.2%, as shown in Table 2. The median duration of treatment was 2.8 months (range, 0.2–25.0 months) and the median number of administered cycles was 3 (range, 1–24 cycles). The chemotherapeutic dose was reduced by 20% to 30% in 68 patients (43.0%). One patient received half the dose of 5-fluorouracil and 75% dose of cyclophosphamide and methotrexate because of hepatic dysfunction due to liver metastasis at the time of initiation or during treatment, and the relative dose intensity was 90.4%.
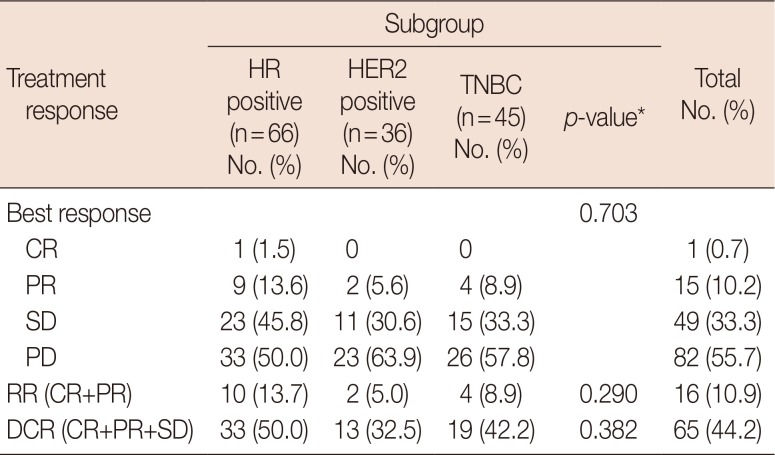
Table 2
Overall response according to subgroup (n=147)
![]()
The DCR was higher in the classic CMF regimen comprising 14 days of daily oral cyclophosphamide with methotrexate and 5-fluorouracil infusion on day 1 and day 8 every 4 weeks than in intravenous CMF every 3 weeks (p=0.015). The DCR was 51.6% (49 patients) in the oral administration group (95 patients) compared to 30.8% (16 patients) in the intravenous administration group (52 patients). The response rate (RR) tended to be superior in the oral administration regimen, but this difference was not statistically significant (13.7% vs. 5.8%, p=0.141). Additionally, the tumor subtype did not affect the DCR and RR after treatment with CMF.
Progression-free survival and overall survival
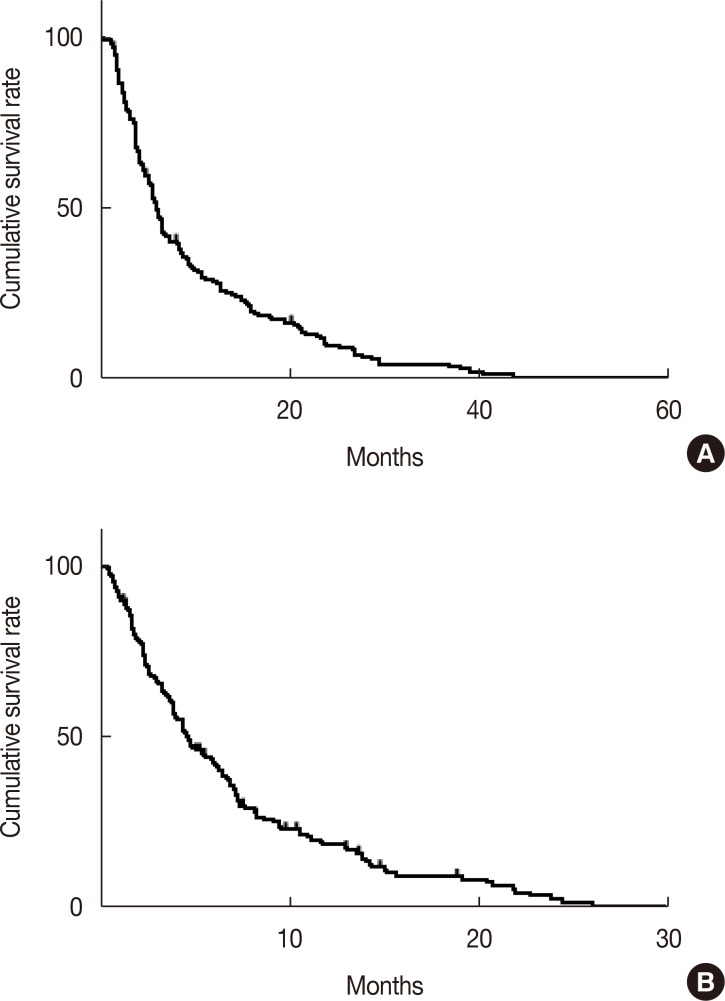
Among the 158 patients, cancer progression or death occurred in 154 (97.4%), and the median PFS was 3.1 months (95% confidence interval [CI], 2.7–3.6). The 6-month PFS rate was 29.4%±3.7% (Figure 1A). The median time to progression was 3.4 months (95% CI, 2.7–4.1). The median OS for all the patients was 9.4 months (95% CI, 7.2–11.6) after initiation of CMF treatment (Figure 1B).
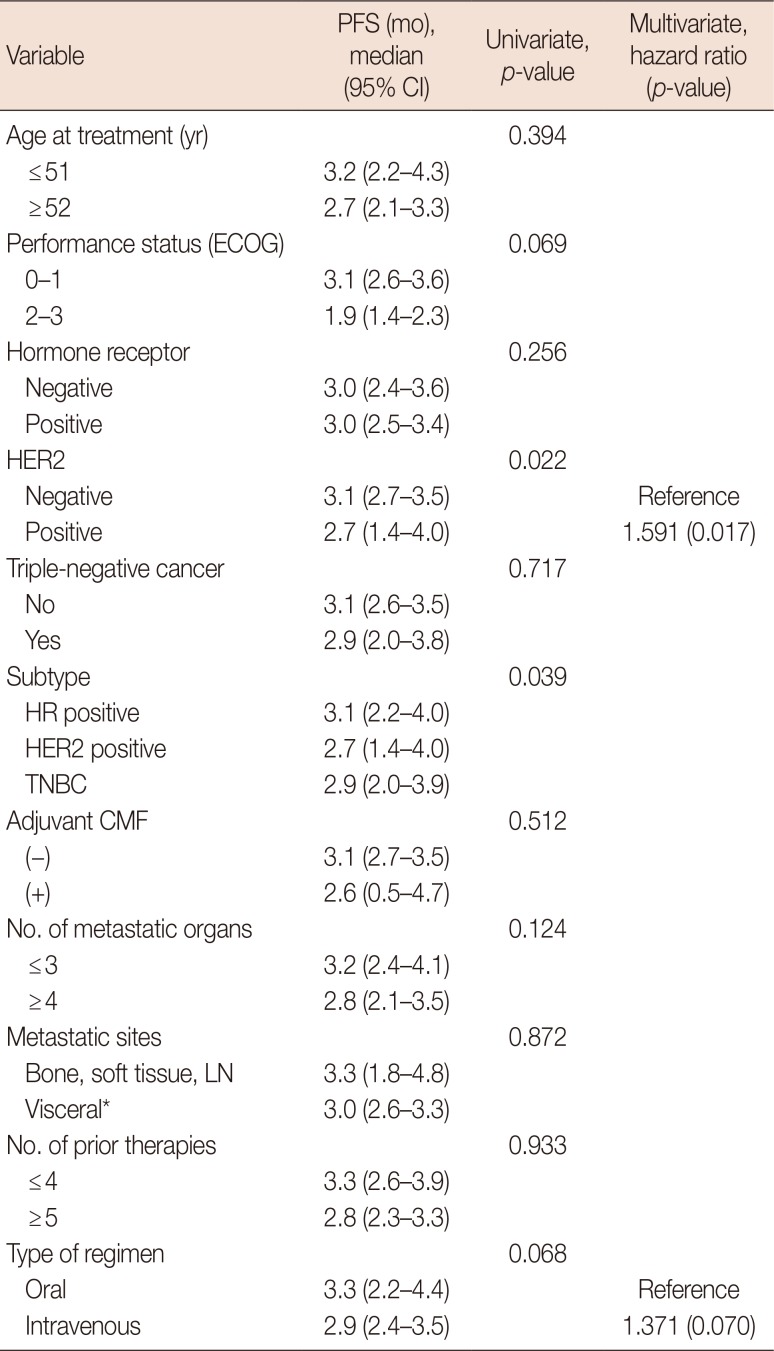
The results of univariate analysis for PFS are shown in Table 3. HER2-negative cancer patients showed longer PFS (3.1 months; 95% CI, 2.7–3.5) compared with HER2-positive cancer patients (2.7 months; 95% CI, 1.4–4.0; p=0.022). In terms of PFS among the three biologic cancer subtypes, the HR-positive subtype (3.1 months; 95% CI, 2.2–4.0) showed superior PFS compared to the HER2-positive group (2.7 months; 95% CI, 1.4–4.0) and the TNBC group (2.9 months; 95% CI, 2.0–3.9; p=0.039) (Figure 2A). The median PFS in 15 patients (9.5%) who received adjuvant CMF was not statistically shorter compared to those who did not receive CMF (2.6 months vs. 3.1 months, p=0.512). Oral CMF regimen improved PFS compared with intravenous CMF every 3 weeks, however the significance was borderline (median, 3.3 months vs. 2.9 months; p=0.068). Other variables, such as the number of metastatic organs (4 or more), poor PS (ECOG 2–3), and dose reduction did not appear to adversely affect the PFS. The median PFS in patients with extensive prior treatment (five or more prior chemotherapy regimens) was not altered compared with PFS of patients treated with less than five prior chemotherapy regimens (median, 2.8 months vs. 3.3 months; p=0.933). For patients who showed CR, PR, and SD, the median PFS was 7.9 months (95% CI, 6.5–9.2), which was longer than the median PFS observed for patients who showed PD as the best response after CMF treatment (1.9 months; 95% CI, 1.8–2.0; p<0.001) (Figure 2B). The median PFS of patients who showed PR and CR was longer compared to patients who showed SD and PD (11.9 months vs. 2.8 months, p<0.001) (Figure 2C). In the multivariate analysis, the oral administration route and HER2 negativity were factors for a favorable PFS (Table 3). Interestingly, the PFS of TNBC patients was similar to that of HR-positive patients, while the PFS of HER2-positive patients was shorter than that of HR-positive patients. This result could be associated with better DCR and RR in HER2-negative patients, although it was not statistically significant.
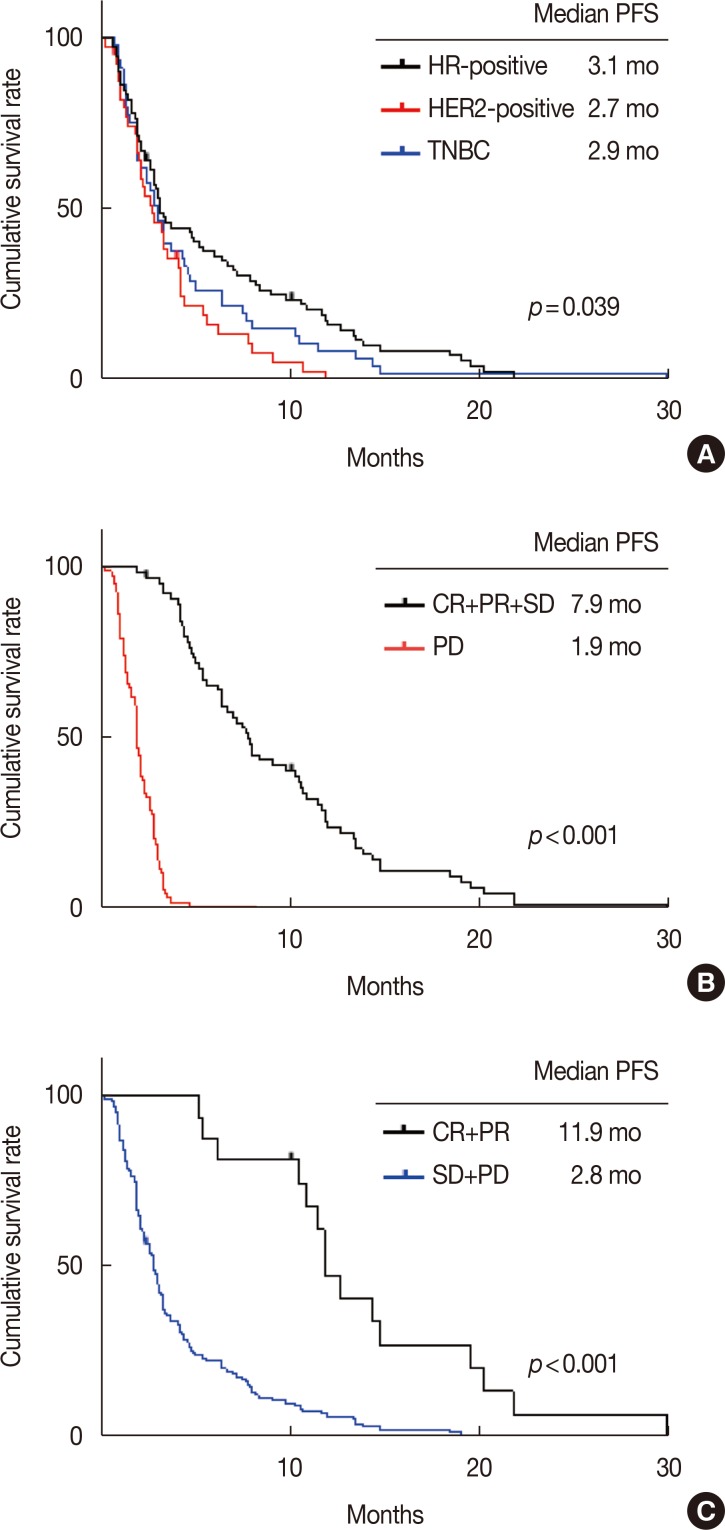 | Figure 2Kaplan-Meier curve of progression-free survival (PFS) based on cancer biologic subtype (A), disease control rate (B), and response rate (C).HR=hormone receptor; HER2=human epidermal growth factor receptor 2; TNBC=triple-negative breast cancer; HR-positive=HR-positive/HER2-negative; HER2-positive=HR-positive or negative/HER2-positive; TNBC=HR-negative/HER2-negative; CR=complete response; PR=partial response; SD=stable disease; PD=disease progression.
|
Table 3
Factors affecting progression-free survival (n=158)
PFS=progression-free survival; CI=confidence interval; ECOG=Eastern Cooperative Oncology Group; HER2=human epidermal growth factor receptor 2; HR=hormone receptor; TNBC=triple-negative breast cancer; CMF=cyclophosphamide, methotrexate, and 5-fluorouracil; LN=lymph node.
*With or without bone, soft tissue, and LN involvement.
![]()
We detected 16 patients with outstanding median PFS of more than 12 months (range, 12.0–54.1 months). No predictive marker for prolonged PFS for CMF was available, except that all 16 patients had HER2-negative disease.
On univariate analysis of the prognostic factors affecting OS, ECOG PS, combined HR and HER2 status (triple-negative status), response to CMF treatment, and the number of metastatic sites were significantly associated with OS (Table 4). The patients presenting with one to three metastatic sites had longer OS compared to those with more than three metastatic sites (median, 11.2 months vs. 3.5 months, p<0.001). The median OS was outstanding in the group with better ECOG PS (ECOG 0–1) compared with the group with worse ECOG PS (median, 9.6 months vs. 4.7 months; p=0.007). HR positivity was a good prognostic marker of OS (median, 10.9 vs. 8.8, p=0.028). Based on the biologic subtype, HR-positive patients had longer OS (12.0 months; 95% CI, 8.5–15.4) than HER2-positive patients (7.0 months; 95% CI, 4.7–9.3) and TNBC patients (8.8 months; 95% CI, 7.2–10.5; p=0.035). The longer median OS in HR-positive patients can reflect favorable RR/DCR, although the median OS was not significantly different between the three groups. The route of CMF administration and number of previous treatment regimens did not affect OS. We also found a strong correlation between achieving treatment response and OS. The median OS in patients with CR, PR, and SD was 15.3 months (95% CI, 12.0–18.6), while the OS in patients with PD was 6.5 months (95% CI, 4.5–8.5; p<0.001). For the patients who showed PR and CR, the median OS was 16.6 months (95% CI, 11.3–21.9), which was longer than that in patients with SD and PD (median, 8.8 months; 95% CI, 7.4–10.2; p=0.010). On multivariate analysis, a small number of metastatic organs (1–3), HR positivity, ECOG PS 0–1, and DCR (SD+PR+CR) were good prognostic factors for OS (Table 4).
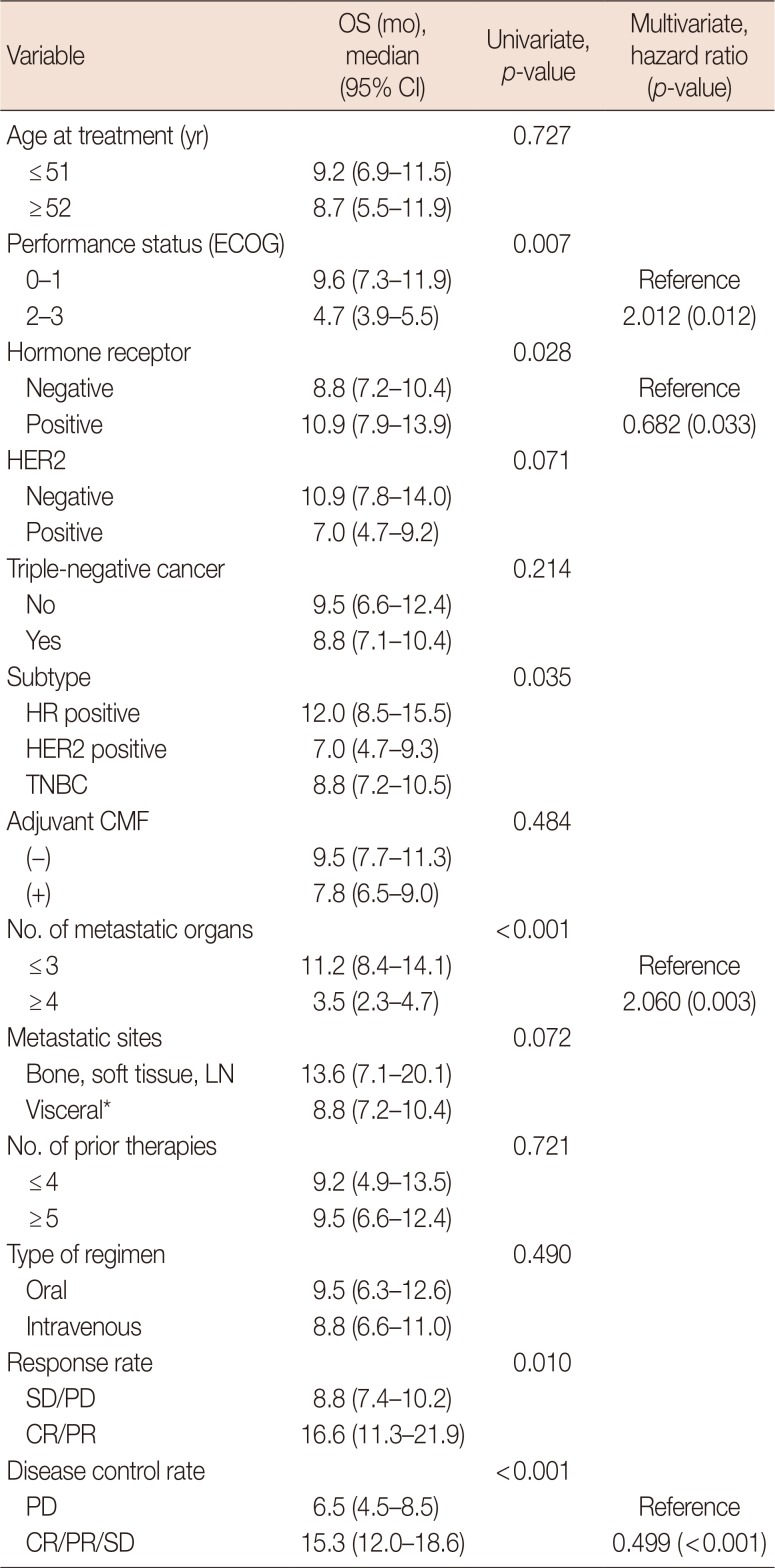
Table 4
Factors affecting overall survival (n=158)
OS=overall survival; CI=confidence interval; ECOG=Eastern Cooperative Oncology Group; HER2=human epidermal growth factor receptor 2; HR=hormone receptor; TNBC=triple-negative breast cancer; CMF=cyclophosphamide, methotrexate, and 5-fluorouracil; LN=lymph node; SD=stable disease; PD=disease progression; CR=complete response; PR=partial response.
*With or without bone, soft tissue, and LN involvement.
![]()
Safety
CMF treatment was associated with a manageable tolerability profile when administered via the oral and intravenous routes. CMF treatment was well tolerated, except in six patients (3.8%) who had to stop chemotherapy due to drug-related toxicity or drug-related morbidities. During treatment, neutropenia, which was the most common toxicity above grade 1, was observed in 47 patients (29.7%). Grades 2, 3, and 4 neutropenia were observed in 11 (7.0%), 26 (16.5%), and 10 patients (6.3%), respectively. The dose delays and reductions were primarily due to neutropenia. Non-hematologic toxicity above grade 2 was not observed.
Go to :
DISCUSSION
This study was motivated by the increasing need for an effective alternative therapeutic strategy for heavily pretreated MBC patients who have failed previous taxanes and anthracycline treatment. Although systemic chemotherapy is effective in advanced breast cancer, the high rate of recurrence and resistance after standard treatment are still the major obstacles in the management of breast cancer patients. Among the conventional cytotoxic agents, taxanes have become the first-line treatment for non-endocrine-responsive and hormone-refractory, non HER2-overexpressing MBC patients, particularly because many of these women have received adjuvant anthracycline. Several options, both single agent and combination regimens, are available as second-line therapy and later for patients with anthracycline- and taxane-resistant disease. Many agents, including gemcitabine, vinorelbine, and fluorouracil, are effective after non-responsive treatment with anthracycline and taxane, which are currently being used in clinical settings [2021222324]. In our study, all except one patient (157, 99.4%) received previous treatment with taxanes, and 154 patients (97.5%) received previous anthracycline-based chemotherapy. Therefore, our population was clinically resistant to both drugs. In addition to taxane- and anthracycline-based chemotherapy, 149 (94.3%), 139 (88.0%), and 138 patients (87.3%) were treated with gemcitabine-, capecitabine-, and, vinorelbine-based chemotherapy, respectively. Patients treated with a median of 5 lines of systemic treatment had a median duration of first-line treatment of 36.0 months (range, 7.1–146.7 months) before the CMF therapeutic regimen. The specific population that we studied had scarce options for systemic treatment at the time that CMF therapeutic was initiated. The evaluation of efficacy of the CMF regimen showed that 16 out of the 147 patients achieved CR or PR and 49 patients had SD. We observed an objective RR of 10.9%, DCR of 44.2%, and a median PFS of 3.0 months, showing that the CMF regimen used was effective in heavily pretreated MBC patients. The treatment outcomes of CMF observed in this study were not inferior to those described for eribulin mesylate, despite that some of our patients were included after eribulin mesylate treatment. In a phase II study, eribulin mesylate was effective for patients with MBC who were previously administered an anthracycline and a taxane, demonstrating RR and PFS of 11.5% and 79 days, respectively [5]. However, this phase II study only included patients with good PS (ECOG 0–1). Meanwhile, our results may better reflect the real-world setting as patients with worse PS were included in our study.
As we expected, all the patients enrolled in our study showed good tolerance to the CMF regimen without fatal toxicity events, and there were restricted cases of toxicity-related drop out. As the quality of life and the symptom palliation for maintaining usual life are the main aims for treatment of advanced MBC patients, a better regimen with safe and tolerable toxicity and not just a moderate efficacy profile needs to be determined. Moreover, cost effectiveness is an advantage of the CMF regimen compared to other targeted agents used in clinical trials. This study provides evidence that the CMF regimen has a good tolerance and safety profile and therefore is a reasonable choice for heavily pretreated MBC patients.
The efficacy of oral CMF and intravenous CMF as adjuvant chemotherapy was demonstrated in randomized trials [1425]. Nevertheless, data regarding the more effective administration route are not available. Our results showed that the DCR and PFS in patients receiving CMF via the oral route were better than in those administered with CMF intravenously. The baseline characteristics between these two groups were not different, and our population was too small to explain why the oral regimen tended to result in a more pronounced response. Additional trials to investigate the differences between oral and intravenous administration of CMF therapy in a palliative setting are planned. Until such studies are performed, we believe that classic CMF regimen have advantages compared to the use of modified intravenous CMF regimen. Recently, there has been a tendency in the chemotherapy industry to create expensive new drugs and discontinue the production of old drugs, such as oral cyclophosphamide. However, our study supported the need for using oral cyclophosphamide chemotherapy for patients with limited therapeutic options.
TNBC comprises 15% to 20% of breast cancer cases and occurs more commonly in young patients [2627]. These clinical cases have an aggressive progression and a higher risk of recurrence and death compared with the non-triple-negative tumor cases [28]. Our study population had a high proportion of TNBC cases (28.5%). Although an aggressive clinical course, poor prognosis, and limited treatment options are associated with TNBC cases, in our study, PFS of the TNBC patients was similar to that of the HR-positive patients. Therefore, CMF combination therapy has shown to be a good therapeutic option for heavily pretreated TNBC patients.
In our study, HER2 positivity adversely affected the median PFS. It was consistent with the results from the Early Breast Cancer Trialists' Collaborative Group meta-analyses that the treatment outcomes of adjuvant CMF was inferior compared to anthracycline-based regimen in HER2-positive cohort [29]. No HER2-positive patient had a median PFS of more than 12 months. To overcome resistance and improve treatment outcomes to CMF, HER2-targeted combination therapy should be considered in HER2-positive patients.
The current study has limitations, particularly the small number of patients and heterogeneity of the population. Additionally, this was a retrospective analysis. Prospective studies are needed to confirm the efficacy of palliative CMF. Nevertheless, our study is the first to provide evidence about the efficacy of the CMF regimen in heavily pretreated MBC patients.
In conclusion, the CMF regimen was not only effective, but also safe for heavily pretreated MBC patients. The oral administration of CMF tented to be more effective than the intravenous route. The PFS in TNBC patients was not inferior to that observed in HR-positive patients. Therefore, CMF can be considered as a reasonable treatment option in patients previously treated with anthracycline, taxanes, and other chemotherapy agents.
Go to :
 XML Download
XML Download