

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is a major health problem and was among the top three most common malignancies globally in 2012 [1]. It is the most common cancer in women, with an estimated 1.67 million new cases diagnosed in 2012 (25% of all cancers in females). It ranks fifth among the most common causes of cancer-related mortality worldwide, while it is the most frequent cause of cancer death in less developed countries [2]. According to the Surveillance, Epidemiology and End Results Program, the 5-year overall survival (OS) of patients diagnosed with breast cancer has been improving steadily over the last 10 years, with death rates falling at a rate of 1.8% per year since 2005. At present, almost 90% of patients diagnosed with breast cancer survive up to 5 years, with survival being strongly associated with the stage at time of diagnosis [3].
Breast cancer is a perfect example of how insights gained from deep understanding of the disease biology can change our approach to its treatment. We have come a long way from treating breast cancer exclusively with morbid radical resections [4] to ultraconservative multimodal approaches, where systemics are combined appropriately with various locoregional treatment modalities, aiming to preserve the local anatomy with positive impact on quality of life (QOL) without compromising the oncologic outcomes. As a staging and therapeutic tool, axillary surgery has traditionally been an integral part of locoregional therapy of breast cancer; however, recent trends have shifted from more radical axillary lymph node dissection (ALND) to a less morbid sentinel lymph node biopsy (SLNB) in those presenting with a clinically negative axilla (cN0). In this paper, we will review the evolution and present status of SLNB in breast cancer.
Go to : 
SIGNIFICANCE OF REGIONAL NODAL INVOLVEMENT IN BREAST CANCER
The significance of tumor lymphatics and their role in tumor progression is debated. Whether the presence of tumor cells in regional nodes is merely a sign of regional progression or an indicator of systemic dissemination of disease is yet to be settled [5]. However, axillary nodal involvement is already established as an indicator of poor prognosis, with the 5-year survival decreasing by approximately 28% to 40% in patients with such a condition [67]. Thus, axillary surgery not only serves as a staging tool but also improves locoregional control, which may result to improved survival.
The role of ALND in patients with cN0 disease has been scrutinized as most of them (70%–80%) will have pathologically free nodes (pN0) [8]. Thus, subjecting these patients to ALND exposes most of them to unnecessary morbid outcomes, such as arm lymphedema, axillary numbness, and shoulder abduction deficits. The role of axillary surgery in cN0 axilla was first evaluated by the National Surgical Adjuvant Breast and Bowel Project (in NSABP B-04 trial) and the Cancer Research Campaign Working Party (King's/Cambridge) [910]. Both these trials showed that treatment of cN0 axilla with either surgery or radiotherapy (RT) did not have any positive impact on OS as compared to observation, and treatment at the time of recurrence. However, both these trials did demonstrate a positive impact of axillary treatment on axillary recurrences in the intervention groups. Driven by this fact and the need to collect information regarding the pathological status of the nodes to identify the candidates for adjuvant chemotherapy, ALND continued to be the standard treatment method for breast cancer until the 1980s. However, as the proportion of patients presenting with cN0 axilla increased, the need for avoiding unnecessary ALND and its morbid sequelae also grew, thus paving way for SLNB in breast cancer.
Go to :
EVOLUTION OF SLNB
Nonsurgical assessment of the axilla has not been promising. Preoperative assessment of the axilla via physical examination has yielded false-negative rates (FNR) of up to 45% [11]. Imaging modalities such as ultrasonography, magnetic resonance imaging, and positron emission tomography/computed tomography have also proven to be of limited value in cN0 axilla staging [121314]. Consequently, surgical staging is the gold standard for assessing the axilla in such patient group.
In the 1940s, studies by Gilchrist [15] and Zeidman and Buss [16] demonstrated that metastatic cells spread through regional lymphatics in an orderly and reproducible manner, thus paving way for the evolution of SLNB. The sentinel lymph node (SLN) is the initial nodes that drains the lymph from a particular organ before draining into subsequent nodes (non-SLNs). Thus, identification and assessment of SLN provides us an accurate clinical window into the regional basin. Before being validated and applied in breast cancer, SLNB was demonstrated to be feasible in parotid tumors, penile cancer, and melanoma [17]. The existence of sentinel node/s in breast was proven by Kett et al. [18] and Krag et al. [19] using two different injection techniques. Further, subsequent studies proved that different areas of the breast drain into the same sentinel node and injection into the dermis or breast parenchyma was immaterial [2021]. The feasibility of identifying SLN in breast cancer and the capability of SLNB to accurately predict the status of the entire axillary basin was demonstrated by Giuliano et al. [22] in 1994.
Go to :
EVIDENCE OF SLNB IN EARLY BREAST CANCER
SLNB in pathologically negative axilla (cN0/pN0)
Several studies evaluating SLNB+ALND using different techniques for lymphatic mapping (blue dye or radiocolloid or their combination) have yielded SLN identification rates of approximately 74% to 94% and FNR up to 13% [23]. A number of randomized controlled trials (RCTs) have compared the rates of disease-free survival (DFS), OS, axillary recurrence, morbidity, and QOL between SLNB alone with SLNB+ALND in patients with pathologically uninvolved SLNs. In most of these studies, the rate of identification of sentinel node was ≥95%, and the FNR was less than 10% [242526272829] (Table 1). The morbidity data also favored SLNB, with significantly less incidence of arm lymphedema, numbness, shoulder movement deficits, and wound seroma noted in patients undergoing SLNB compared to ALND (Table 2) [242527303132]. The survival statistics from these trials did not reveal any negative impact of SLNB on regional recurrence, DFS, or OS (Table 3) [2529303334]. Two recent meta-analyses, which included all the major RCTs, that assessed the efficacy of SLNB in pathologically free axilla (pN0) further reinforced the favorable impact of SLNB on morbidity and equivalent oncological outcomes [3536]. Moreover, the positive impact of SLNB on patient reported outcomes was also confirmed in these trials. Based on these trials and other related evidence, the American Society of Clinical Oncology (ASCO) recommended SLNB in clinically early breast cancer (T1/T2) with cN0 axilla in their recently published clinical practice update [37].
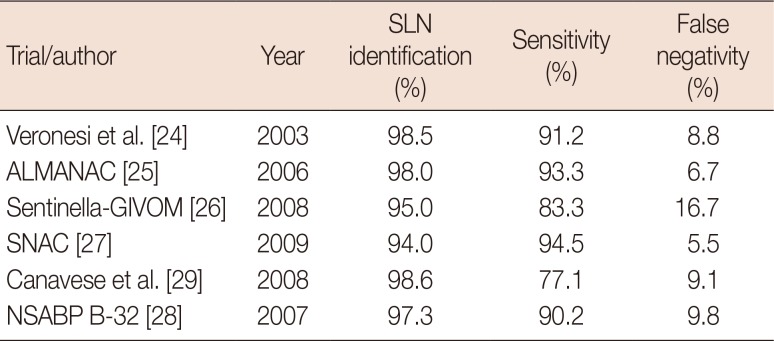
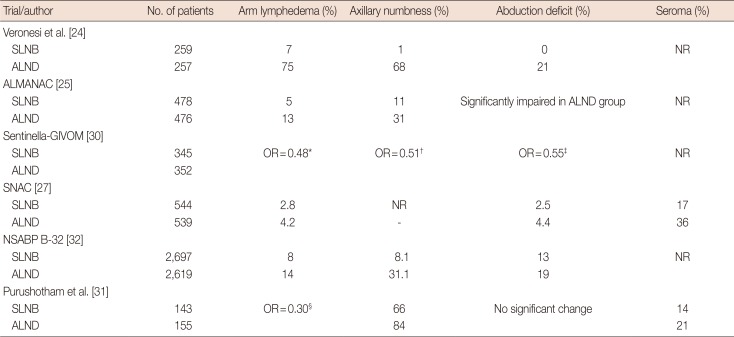

Table 1
Accuracy of sentinel node biopsy in early breast cancer
| Trial/author | Year | SLN identification (%) | Sensitivity (%) | False negativity (%) |
|---|---|---|---|---|
| Veronesi et al. [24] | 2003 | 98.5 | 91.2 | 8.8 |
| ALMANAC [25] | 2006 | 98.0 | 93.3 | 6.7 |
| Sentinella-GIVOM [26] | 2008 | 95.0 | 83.3 | 16.7 |
| SNAC [27] | 2009 | 94.0 | 94.5 | 5.5 |
| Canavese et al. [29] | 2008 | 98.6 | 77.1 | 9.1 |
| NSABP B-32 [28] | 2007 | 97.3 | 90.2 | 9.8 |
![]()
Table 2
Comparison of morbidity outcomes (SLNB vs. ALND)
| Trial/author | No. of patients | Arm lymphedema (%) | Axillary numbness (%) | Abduction deficit (%) | Seroma (%) |
|---|---|---|---|---|---|
| Veronesi et al. [24] | |||||
| SLNB | 259 | 7 | 1 | 0 | NR |
| ALND | 257 | 75 | 68 | 21 | |
| ALMANAC [25] | |||||
| SLNB | 478 | 5 | 11 | Significantly impaired in ALND group | NR |
| ALND | 0476 | 13 | 31 | ||
| Sentinella-GIVOM [30] | |||||
| SLNB | 345 | OR = 0.48* | OR = 0.51† | OR = 0.55‡ | NR |
| ALND | 352 | ||||
| SNAC [27] | |||||
| SLNB | 0544 | 2.8 | NR | 2.5 | 17 |
| ALND | 0539 | 4.2 | - | 4.4 | 36 |
| NSABP B-32 [32] | |||||
| SLNB | 2,697 | 8 | 8.1 | 13 | NR |
| ALND | 2,619 | 14 | 31.1 | 19 | |
| Purushotham et al. [31] | |||||
| SLNB | 143 | OR = 0.30§ | 66 | No significant change | 14 |
| ALND | 155 | 84 | 21 |
![]()
Table 3
Comparison of survival outcomes (ALND vs. SLNB)
| Trial/author | Axillary recurrences (%) | Disease-free survival (%) | Overall survival (%) |
|---|---|---|---|
| Veronesi et al. [33] | 0 vs. 0.01 | 88.8 vs. 89.9 (10 yr)* | 89.7 vs. 93.5 (10 yr)† |
| ALMANAC [25] | 0.84 vs. 0.2 (1 yr) | NR | NR |
| Sentinella-GIVOM [30] | 0.05 vs. 0.01 | 89.9 vs. 87.6 | 95.5 vs. 94.8 |
| Canavese et al. [29] | 0.87 vs. 0.0 | 89.8 vs. 94.5‡ | 97.2 vs. 97.2§ |
| NSABP B-32 [34] | 0.1 vs. 0.3 | 82.4 vs. 81.5 (8 yr) | 91.8 vs. 90.3 (8 yr) |
![]()
SLNB in pathologically positive axilla (cN0/pN+)
SLNB has been established as the standard pathological diagnostic tool for the cN0 axilla. Pathologists have used new technologies such as serial sectioning, immunohistochemistry (IHC), and molecular techniques, including polymerase chain reaction, for detecting disease in these nodes that would have otherwise gone unnoticed on routine histopathological examination (HPE). This has led to the detection of metastases in up to one-third of patients who were otherwise categorized as pN0 on routine HPE [38]. The American Joint Committee on Cancer has incorporated these changes by categorizing nodal metastases into three groups: (1) isolated tumor cells (ITCs): when no cluster is >0.2 mm, pN0 [i+]; (2) micrometastasis: 0.2 to 2.0 mm, pN1mi; and (3) macrometastasis: >2.0 mm [39].
The significance of these small deposits (ITCs and micrometastasis) has been long debated. In a Dutch retrospective study (MIRROR trial), the outcome of patients with pN0 disease was compared with those having ITCs or micrometastases, and the results indicated a negative impact of the latter on the DFS of these patients [40]. The prognostic impact of ITCs and micrometastases has been the subject of two large trials, the American College of Surgeons Oncology Group (ACOSOG) Z0010 and NSABP-32 trials. In the ACOSOG Z0010 trial, which is a prospective observational study, occult metastases were detected on immunohistochemical examination in sentinel nodes of an additional 10.5% of patients who were otherwise reported negative on routine HPE; further, this did not translate into worse survival in patients with cT1/T2 N0M0 disease [41]. Thus, routine IHC in SLN was not supported by this study. Meanwhile, NSABP B-32 is the largest trial conducted assessing the efficacy of SLNB in early breast cancer. In this trial, IHC detected occult metastases in an additional 15% to 16% of patients who had otherwise negative SLNs on routine HPE. However, the presence of occult metastasis in the sentinel nodes was not a negative prognosticator for OS [34], thus corroborating the findings of the ACOSOG Z0010 study.
Several studies have demonstrated that approximately 34.3% to 85.7% of patients with sentinel node metastases will have no additional nodal disease [38]. If the sentinel nodes harbor micrometastases or ITCs, then the risk of involvement of additional nodes is even less (20% and 12%, respectively) [4243]. This makes the rationale of doing completion ALND even in patients with positive SLNs questionable as most of them will have no additional nodal burden. In two different large retrospective studies, 16% and 20.8% of patients with positive SLNs did not undergo completion ALND, and this did not have any negative impact on their axillary failure rates and OS [4445]. However, being retrospective in nature, these studies suffer from selection bias. Two RCTs compared observation versus ALND in patients with early breast cancer and limited occult axillary disease.
First was the ACOSOG Z0011 study that was a phase 3 noninferiority trial in which patients with T1 or T2 carcinomas undergoing breast-conserving surgery (BCS), with one or two positive sentinel nodes, were randomized either to completion ALND (n=445) or observation (n=446) [4647]. All patients were supposed to receive adjuvant radiation through tangential fields. Almost all patients received systemic chemotherapy with or without hormone therapy. Although target enrolment was 1,900 patients, this trial was closed early due to slow accrual and very low event rate. After a median follow-up of 6.3 years, the 5-year OS was 91.8% in the ALND arm and 92.5% in the observation arm (p=0.008 for noninferiority). Similarly, the 5-year DFS was 82.2% for patients undergoing ALND and 83.9% for those subjected to SLNB only. Regional recurrences were also similar in both groups (0.5% in ALND and 0.9% in SLNB alone). Although the results of this trial were provocative, it has been criticized for various reasons. It failed to achieve its accrual goal of 1,900 patients and was able to recruit only 891 patients. However, due to the low accrual rate and lower–than-expected event rate, even if the target 1,900 patients would have been recruited, it would have taken more than 20 years of follow-up to observe the 500 deaths needed for giving 90% power to confirm noninferiority of SLNB alone over ALND. Thus, in spite of this, the authors maintained that predefined statistical analysis was able to demonstrate noninferiority of SLNB alone over ALND [48]. This trial also has been criticized for violation of protocol guidelines for irradiation in a significant number of patients. Although patients were supposed to receive whole breast radiation through only two tangential fields (with no planned axillary radiation), the tangential fields in some patients had been extended cranially to cover the undissected axilla. In addition, 18.9% of patients received three fields of radiation [49]. These and many other questions related to this trial have been answered in subsequent publications [50].
The other trial was conducted by the International Breast Cancer Study Group (IBCSG 23-01) and corroborated the findings of the Z0011 trial. It was a noninferiority trial in which patients with cN0, T1/T2 disease and having ≥1 positive sentinel nodes with micrometastases were randomized to either ALND or observation groups [51]. Unlike the Z0011 trial, patients could undergo mastectomy or BCS. Similar to Z0011, this trial was terminated early due to slow accrual. Only 934 patients were recruited against the planned target of 1,960 patients. The radiation fields were not defined in this trial, and 9% of patients in each group did not receive any radiation. After a median follow-up of 5 years, the 5-year DFS was 87.8% in the observation group and 84.4% in the ALND group (hazard ratio, 0.78; 95% confidence interval [CI], 0.55–1.11; p=0.004 for noninferiority). The 5-year OS was 97.6% in the ALND group, and 97.5% in the observation group (logrank p=0.73). Regional recurrence rates in the ALND and observation group were 0.2% and 1%, respectively. As in the previous trials, the authors of this trial also concluded that ALND can be safely omitted in patients with micrometastatic nodal disease. In a meta-analysis of 12 studies (five randomized and seven observational), which comprised 130,575 patients with early breast cancer and positive sentinel nodes, patients who underwent SLNB alone (n=26,870) were found to have minimal adverse effects profile and similar oncological outcomes as compared to those who underwent ALND (n=103,705) [52].
The results of the Z0011 and IBCSG 23-01 trials have been incorporated into daily practice by many large academic cancer institutions and community-based breast surgeons. In an electronic survey conducted among members of three different surgical societies of the Pacific Northwest, 181 respondents reported performing few completion ALNDs (61%), few intraoperative frozen sections (21%), and no IHC (12%), because of the above trial data [53]. In another study, investigators from the MD Anderson Cancer Centre reviewed the practice patterns in patients fulfilling the inclusion criteria of the Z0011 trial and noted that few patients underwent completion ALND (85% in pre-Z0011 era compared to 24% in post-Z0011 period) and intraoperative nodal assessment (26% vs. 69%, p<0.001) after the results of the Z0011 trial were discussed in institutional multidisciplinary meetings [54]. In another Dutch study, data (covering the period from January 1993 to July 2014) from a population-based cancer registry of the South Netherlands was assessed, and the results showed that 34,037 patients staged via SLNB without completion ALND increased from 0% in 1993–1994 to 69% in 2013–2014. In the same period, the proportion of patients undergoing ALND decreased from 88.8% to 18.7% [55]. Similar changes in practice have also been confirmed by other reports [5657].
Go to :
SLNB AFTER NEOADJUVANT CHEMOTHERAPY
Neoadjuvant chemotherapy (NACT) is a standard initial treatment in patients with locally advanced breast cancer and in those with large primary tumors to facilitate breast conservation. NACT downstages the disease in most patients, with complete pathological response being achieved in 20% to 50% of patients [5859], and can reach up to 60% with the use of anti-human epidermal growth factor receptor 2 (anti-HER2) therapies [60]. Although ALND has been the standard treatment modality in this setting, SLNB can potentially spare many of these patients from extensive axillary surgery. Concerns regarding poor identification and high FNR (up to 30% in some studies) in this setting have been expressed [146162]. NACT and SLNB (upfront or post-NACT) sequencing has been debated extensively, with each approach having its advantages and disadvantages [5859]. The strongest advantage of upfront SLNB is that the pathological status of the axilla is known beforehand, which can have therapeutic implications on locoregional treatment, mainly RT. The main concern regarding SLNB post NACT is the poor identification rate of SLN due to possible alteration of lymphatics as a result of NACT. Another concern is the high FNR because upfront chemotherapy may show different effects on sentinel and non-sentinel nodes; the malignancy may be eradicated in sentinel nodes, while residual disease may persist in non-sentinel nodes.
SLNB in clinically negative axilla (cN0)
The debate of upfront versus post-NACT SLNB is relevant in patients with clinically negative axilla. Many previous studies have shown SLN identification rates of 72% to 100% and FNR up to 33% [59] after NACT. NSABP-27 was a multicenter study in which a subset of 428 patients underwent SLNB+ALND after NACT [62]. The reported SLN identification rate was 85% and the FNR was 11%, with the FNR being lower with radio-isotope (8%) than with blue dye (14%). This study included patients with cN0 and cN+ axillary nodes before NACT, but the FNR was not significantly different between these two groups (12.4% vs. 7%, respectively, p=0.51). In another French multicenter study (GANEA), which evaluated 195 patients with T0-3N0-1 breast cancer with dual lymphatic mapping after NACT, the SLN identification rate and FNR were reported to be 90% and 11.5%, respectively [63]. A number of meta-analyses combining data on cN0 and cN+ patients have reported the FNR for SLNB after NACT to be between 10.5% and 15.1% [646566]. The SLN identification rates in these meta-analyses were in the range of 90%. In another meta-analysis that only included patients with cN0 axilla, the SLN identification rate was as high as 94.3% and the FNR was 7.4% [67], which is not different from the data on SLNB reported in early breast cancer.
In a population-based study, van der Heiden-van der Loo et al. [68] compared SLNB in patients with cN0 axilla before NACT (n=980) and post-NACT (n=203). They reported that patients who underwent SLNB after NACT had a higher chance of having negative SLN than those who underwent SLNB before NACT (67% vs. 54%, p=0.001) and had lesser chance of undergoing ALND (33% vs. 45%, p=0.006) [68]. Collectively, these results indicate that SLNB after NACT in patients with cN0 axilla is a feasible treatment option, and additional axillary treatment is not necessary in those with negative SLN.
SLNB in clinically positive axilla (cN+)
The status of SLNB in patients with cN+ axilla who achieve complete clinical response (ycN0) after NACT is controversial. Initial studies evaluating SLNB in this setting have revealed high FNR of >25% [6970]. In a large retrospective study, the identification rate of SLN after NACT was significantly low (77.6%), although FNR was comparable to upfront approach [71]. A recent meta-analysis of 1,395 patients with cN1 axillary disease reported an SLN identification rate after NACT of 92.3% (90.8%–93.7%) and FNR of 15.1% [72]. Further, this meta-analysis showed lower SLN identification rate with the use of blue dye alone than radiotracer or a combination of these techniques.
Three recent prospective observational studies, namely, ACOSOG Z1071, SENTINA, and SN FNAC, have provided additional insights in this subject [737475]. These three studies had slightly different designs, but all of them evaluated SLNB in patients with cN+ axilla who achieved ycN0 status after NACT (Table 4). The following conclusions can be drawn from these studies to optimize SLNB after NACT: (1) use of dual tracer lymphatic mapping; (2) identification and retrieval of >2 SLNs; (3) use of IHC for disease detection in SLNs; and (4) performance of completion ALND in patients with pN(i+) disease.
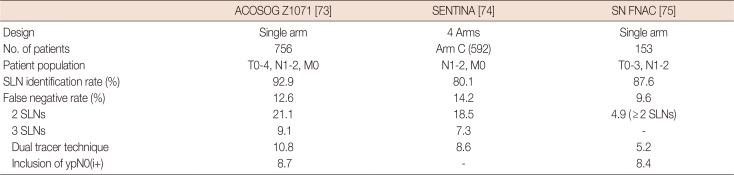
Table 4
Summary of prospective studies of sentinel node biopsy after neoadjuvant chemotherapy in cN+ axilla
| ACOSOG Z1071 [73] | SENTINA [74] | SN FNAC [75] | |
|---|---|---|---|
| Design | Single arm | 4 Arms | Single arm |
| No. of patients | 756 | Arm C (592) | 153 |
| Patient population | T0-4, N1-2, M0 | N1-2, M0 | T0-3, N1-2 |
| SLN identification rate (%) | 92.9 | 80.1 | 87.6 |
| False negative rate (%) | 12.6 | 14.2 | 9.6 |
| 2 SLNs | 21.1 | 18.5 | 4.9 ( ≥ 2 SLNs) |
| 3 SLNs | 9.1 | 7.3 | - |
| Dual tracer technique | 10.8 | 8.6 | 5.2 |
| Inclusion of ypN0(i+) | 8.7 | - | 8.4 |
![]()
Various methods have been suggested to lower FNR of SLNB after NACT. These include (1) identification and clip placement in positive node before starting NACT and removing the clip-bearing node after completion of NACT; (2) marking the axillary nodes with radioactive iodine seeds (MARI procedure) to assess the response of nodal disease to NACT; or (3) tattooing the positive nodes before starting chemotherapy [59]. In its latest update on SLNB in breast cancer, considering all the available data, the ASCO has recommended that SLNB may be offered in patients with operable breast cancer before or after NACT, with supporting data showing that the procedure is less accurate after NACT [37].
Go to :
OTHER INDICATIONS
Ductal carcinoma in situ
Ductal carcinoma in situ (DCIS) currently comprises up to 20% of newly diagnosed cases of breast cancer [7677], with more than 80% of these being detected via mammogram [78]. Theoretically, DCIS being a noninvasive disease has no potential of spread via lymphovascular route; however, up to 26% of the patients diagnosed via needle biopsy may harbor invasive or microinvasive disease on final histopathology [79]. Further, approximately 2% to 14% of patients diagnosed with DCIS harbor positive SLNs on final histopathology because the presence of invasive component in the lesion is not determined on initial tissue sampling [80818283848586]. Multiple factors, including palpability, mammographic size >4 cm, high grade, age <55 years, diagnosis on smaller core biopsy needle, and multicentricity, may help predict an increased risk of invasive or microinvasive component in the final specimen [8387].
Although routine SLNB is not recommended in DCIS, some associations, such as the National Comprehensive Cancer Network and ASCO, recommend its selective use in certain situations, including in those undergoing mastectomy, when lesion is located at a site that precludes future SLNB, when the lesion is palpable on examination, when imaging is highly suggestive of invasive lesion, and when the area of DCIS is greater than 5 cm [3788].
Multicentric lesions
Multicentric tumors can occur in up to 10% of patients with breast cancer. A theoretical concern that different lesions may drain into different SLNs, hence making SLNB unreliable in this situation has been expressed. A >95% SLN identification rate has been reported by several retrospective studies [899091], and most studies have reported an FNR of less than 9% in this setting [92]. Further, the rate of axillary recurrence reported in these studies is similar to that in unicentric lesions [9091]. Hence, SLNB can be offered in patients having multicentric disease with cN0 axilla.
Prophylactic mastectomy
Prophylactic mastectomy (PM) can be offered to reduce the risk of cancer in women with a family history of breast and ovarian cancer or in those with known oncogenic BRCA mutation and is even chosen by those who have a history of breast cancer on the contralateral side. At present, the rates of PM have increased in Western countries [9394]. Pathological studies of mastectomy specimens in these patients have reported a 3.5% to 5% incidence of occult cancer [9596].
The data on SLNB during PM are only from few retrospective studies, which have reported low rates of sentinel node positivity. In a recent meta-analysis of six retrospective studies comprising 1,251 patients undergoing 1,343 prophylactic mastectomies, occult cancer was found in 21 of specimens (1.7%), and a positive SLNB was detected in 23 of patients (1.9%). Of these 23 patients with positive SLNB, approximately half had locally advanced malignancy in the contralateral breast [97]. In another meta-analysis of 14 studies comprising 2,708 prophylactic mastectomies, the rates of occult carcinoma and positive SLNs were 1.8% (n=51) and 1.3% (n=33), respectively. Similar to a previous review, most patients with positive SLNs had a locally advanced disease in the contralateral breast [98]. Thus, routine use of SLNB during PM cannot be recommended as it would lead to unnecessary morbidity and additional costs; however, selective use of SLNB may be considered in those with a high risk of harboring an occult malignancy in PM [99].
Previous axillary or breast surgery
With the advances in therapeutic management, patients with breast cancer achieve long survival rates, and approximately only 5% to 10% will develop local recurrence in the breast or chest wall over a long period [100101]. In a recent meta-analysis, the overall locoregional recurrence rate was 7.9%, with the rate being 8.95% after mastectomy and 7.12% after BCS [102]. The standard treatment in these patients was re-excision or salvage mastectomy with ALND. However, in most of these patients with cN0 axilla, positive nodes were found only in up to one-fourth of patients [103104]. As such, most of them were subjected to unnecessary ALND. SLNB has the potential to avoid unnecessary axillary surgery and also help us in deciding about adjuvant therapy. However, a potential problem associated with SLNB in the setting of previous axillary intervention (ALND or SLNB) and/or adjuvant RT is aberrant lymphatic drainage, which can compromise the safety and accuracy of this procedure.
In a meta-analysis of 25 studies comprising 692 patients with locally recurrent breast cancer, aberrant lymphatic drainage was noted in 43.2% of patients and was seen more frequently after previous ALND than after previous SLNB (69.2% vs. 17.4%, p<0.0001). The sentinel node identification rate was 65.3%, which was significantly higher in those who had previous SLNB than those who had previous ALND (81.0% vs. 52.2%, p<0.0001). In these patients who underwent previous SLNB, 19.2% of sentinel nodes was positive for metastases, and 27.5% of these were located in the aberrant lymphatic basin. Importantly, data collected via SLNB changed the adjuvant treatment decisions in 17.9% of patients [104]. In a more recent meta-analysis of seven studies reporting data on lymphatic mapping in 1,053 patients with recurrent breast cancer, the SLN identification rate was 59.6% (95% CI, 56.7%–62.6%), which was significantly higher in those who had SLNB as original axillary surgery as than those who had ALND (odds ratio, 2.97; 95% CI, 1.66–5.32). Aberrant lymphatic drainage was noted in 25.7% (23%–28%), which was significantly higher in those who initially underwent ALND than SLNB. Sentinel node was harboring disease in 10.4% (8.6%–12.3%) of patients, and a positive sentinel was commonly located in the ipsilateral axilla [105].
These findings show that SLNB (preferably via dual mapping technique) is feasible in recurrent breast cancer and can help us in avoiding ALND in >50% of patients. It can potentially help clinicians to identify regional metastases outside the ipsilateral axilla and allow patients to receive targeted surgical and adjuvant therapies. However, its benefit on recurrence and survival is unknown; as such, large RCTs with long follow-up are needed.
Go to :
CONTRAINDICATIONS
At present, data are insufficient to recommend SLNB in large T4 tumors, inflammatory breast cancer, and clinically palpable metastatic axillary nodes. Further use of blue dyes has not been proven safe in pregnancy; moreover, data on the effects of radiotracer on developing fetus is limited, rendering pregnancy a contraindication for SLNB [37].
Go to :
CONCLUSION
Sentinel node biopsy is the current paradigm in the management of regional basin in breast cancer. With continuous improvement in cure rates over the last few decades, limiting surgery and maintaining QOL have become important concepts in the management of breast cancer. SLNB has proven to be an efficacious and cost-effective tool in breast cancer. Its application has expanded beyond early breast cancer, and it has been established in areas where it was previously considered inapplicable. For instance, SLNB is gradually incorporated in the management of patients with cN+ axilla who are rendered cN0 after NACT.
Go to :
 XML Download
XML Download