

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In Argentina, breast cancers have the highest incidence and mortality in women [1]. Seventy percent of these tumors are hormone-dependent, and the expressions of estrogen receptor (ER) and progesterone receptor (PR) are considered as prognostic and predictive factors. The overexpression of the human epidermal growth factor receptor 2 (HER2) occurs in 20% of these tumors, and its positive expression has important therapeutic implications. Treatment decisions are based on the clinical, histological, and immunohistochemical information obtained from the analysis of these tumors [2]. Nodal status is considered an indicator of tumor chronology; patients with node-negative cancers are believed to demonstrate better prognoses, although some authors may describe this as “lead time bias” [3]. However, nodal status is considered a marker of tumor phenotypes because this factor retains its prognostic importance after patients undergo relapses.
Several studies have shown that the expressions of the ER, PR, and HER2 may vary during tumoral progression and development of metastases [45]. Consequently, in several clinical scenarios, conducting biopsies of metastases is recommended, to adequately define their phenotypes and subsequent treatments [6]. Similarly, differences in the expressions of these receptors may be expected between primary breast tumors and synchronic nodal metastases [7].
In this study, we aimed to describe and compare the expressions of ER, PR, and HER2 in primary breast tumors and synchronic axillary nodal metastases, and evaluate the phenotypic alterations between these neoplastic tissues.
METHODS
Patient population
Patients were identified prospectively from the surgical procedures for breast cancers at the Alexander Fleming Institute between September 2013 and July 2016. Inclusion criteria included patients who (1) were older than 18 years, (2) signed informed consents, and (3) presented with synchronic axillary nodal metastases after undergoing therapeutic breast surgeries and axillary procedures. This study was approved by the Institutional Review Board (No. 725). They received treatments based on their pathologies, following international and institutional standards. Our analysis did not affect any diagnostic and therapeutic decisions.
Pathological analysis
During gross examinations, the sentinel lymph nodes >4 mm in diameter were bisected. Frozen sections were obtained, and the nodes were processed in individual blocks for the preparation of permanent sections and histopathologic evaluations using hematoxylin and eosin (H&E) staining. If the tumor could not be identified using H&E staining, then cytokeratin (Clone AE1-AE3; Dako, Glostrup, Denmark) immunohistochemistry (IHC) was performed, at one level (in a total of two faces in a bisected node) along with routine histologic examination of the sentinel lymph nodes using H&E. Thus, a sentinel node was examined in three sections (six faces): (1) frozen, (2) H&E stained, and (3) IHC stained. Cytokeratin immunostaining was considered positive, if the lymph node contained immune-reactive cells that appeared malignant or if there were cytologically atypical individual cells with strong cytokeratin reactivity in subcapsular sinuses. The cytokeratin IHC staining was reviewed independently by two pathologists [8].
We selected slides with greater amounts of tumor tissue, after a lymphatic mapping, as described above, for the analysis of ER (Clone 6F11; Leica Biosystems, Nussloch, Germany), PR (Clone 16; Leica Biosystems), and HER2 (Clone SP3; Cell Marque, Rocklin, USA). HER2 staining was interpreted as follows: membrane staining in 10% of invasive tumor cells was considered positive, when scoring for HER2. The IHC scoring method for HER2 was a semiquantitative method based on the intensities of the reaction products and the percentages of membrane-positive cells, yielding a score range of 0 to 3+. A score of 3+ was regarded as unequivocally positive, and scores of 0 or 1+, as negative. Borderline scores (2+) were regarded as equivocal, and fluorescence in situ hybridization was performed for those cases [9].
Classification
Hormonal receptors (HRs) were analyzed in terms of their percentages of expression; expressions >1% were considered positive. Overexpression of HER2 was considered positive, if more than 10% of tumor cells showed the presence of homogeneous and dark circumferential (chicken-wire) patterns.
Phenotypically, tumors and metastases were classified as follows: luminal A, if ER+, PR ≥20%, or Ki-67 ≤20%; luminal B, if ER+, PR <20%, or Ki-67 >20%; luminal B/HER2, if HR+ and HER2+; HER2, if HR− and HER2+; and triple negative, if HR− and HER2−
Statistical analysis
Categorical variables were expressed as absolute numbers and percentages. Continuous variables were described in terms of means and standard deviations if normally distributed, or medians and interquartile ranges otherwise. Comparison between groups were conducted using the Student t-test and the Wilcoxon rank sum test for continuous variables, and the chisquare test and Fisher exact test for categorical variables. Interrelationships between two continuous variables were examined using the Spearman's correlation. Bland-Altman plots were obtained for concordance analysis of continuous variables and Cohen's κ coefficient, for that of categorical variables. The relationships between each of the variables and the phenotype alterations were assessed individually using univariate analysis. The variables that were assessed as statistically significant using univariate analysis were included in multivariate analysis. Multivariate logistic regression was used to determine factors predictive of phenotype alterations. A p-value < 0.05 was considered statistically significant. Statistical analysis was carried out with Statistix 8.0 (Analytical Software, Tallahassee, USA).
RESULTS
During the period of study, 127 patients presented with synchronic axillary nodal metastases. The complete analysis of HR and HER2 in primary tumors and nodal samples was carried out in 118 patients. A summary of baseline characteristics is shown in Table 1.
Correlation between hormonal receptors and Ki-67 in breast tumors and nodal metastases
Correlation analysis between HRs and Ki-67 showed statistical dependence between these variables. Patients with high expressions of ER in primary breast tumors presented with high expressions of ER in nodal metastases (Spearman's rho 0.77, p<0.001). Similar dependence was observed between PR (Spearman's rho 0.81, p<0.001) and Ki-67 (Spearman's rho 0.72, p<0.001). The scatter plots shown in Figure 1 illustrate these relationships.
To adequately analyze the concordance between HRs and Ki-67 in both sets of samples, Bland-Altman plots were obtained for each determination (Figure 2).
Phenotypic alterations between breast tumors and nodal metastases
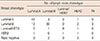
Primary breast tumors were classified into five subgroups according to their immunohistochemical analysis: luminal A constituted 41.6% of the tumors; luminal B, 40.0%; luminal B/HER2, 9.6%; HER2, 2.4%; and triple negative, 6.4%. Nodal metastases were classified as follows: luminal A, 50.8%; luminal B, 30%; luminal B/HER2, 7.5%; HER2, 6.7%; and triple negative, 5%. The phenotypic correlation between these subgroups is shown in Table 2. Alterations of phenotypes between primary breast tumors and nodal metastases were observed in 28% of the patients. The most frequently observed alteration was from a luminal B subtype to a luminal A subtype (36.4%, n=12). Alterations with therapeutic implications occurred in 10 cases (30.3%); six showed overexpression of HER2 in nodal metastases that was not detected in the primary breast tumors, and four gained HR expression.
The number of observed agreements was 86 (72.9% of the observations). Nevertheless, 33.8% of these agreements could have occurred by chance. The Cohen's κ coefficient indicated a moderate strength of agreement (κ, 0.59; 95% confidence interval, 0.48–0.71).
Analysis of factors associated with phenotypic alterations
Clinical and pathological factors were analyzed, to describe their associations with the phenotypic alterations in nodal metastases. In univariate analysis, high histological grade and high Ki-67 expression showed associations with variations in the classification of phenotypes. In multivariate analysis, high histologic grade (odds ratio [OR], 2.79; p<0.047) and high Ki-67 expression (OR, 1.05; p<0.037) remained independent factors that were predictive of phenotypic alterations. The results of the analysis of all factors are shown in Table 3.
DISCUSSION
Intratumoral heterogeneity is a recognized characteristic of breast neoplasms, in genetic, proteomic and macroscopic levels. Furthermore, heterogeneity exists between primary tumors and the corresponding metastases [10]. It is known that tumors may differentiate as they metastasize, changing their biological characteristics. The metastatic outcomes are dependent on a selection process that favors the survival and growth of a distinct special subpopulation of cells. The main purpose of investigating this heterogeneity is to evaluate its effects on prognosis and the efficacy of therapy.
Axillary nodes are the first sites of metastasis in breast cancers. Cells from these sites may represent the ones with greater invasive and proliferative capacities, and may be responsible for the occurrence of distant metastases. Between primary breast cancer and metastases, published literature reflects a discordance of 15% to 54% in HRs [61112], and up to 34% in HER2 [61213]. When the data is restricted exclusively to alterations in axillary nodal metastases, this discordance varies from 10% to 30% for HRs, and 10% to 20% for HER2 [141516]. Comprehensive comparisons of biomarker expressions between primary breast carcinomas and the corresponding metastatic carcinomas in patients, as well as that between different metastatic sites from the same patient showed heterogeneous expressions of these biomarkers. In this report, the therapeutic targets identified in the primary breast carcinomas, or even in some metastatic breast carcinomas might not reflect the targets present universally in all metastatic sites [17].
In our study, a significant correlation was observed in the expressions of HRs and Ki-67 between primary breast tumors and axillary nodal metastases, and moderate concordance was observed in the phenotypic characteristics of these two different neoplastic tissues. This may support the argument for avoiding the use of immunohistochemical analysis, in this scenario. Nevertheless, as described earlier, phenotypic changes did exist between the two samples (28% in the patients in our study). One-third of these changes have therapeutic implications implications, thus adding more effective tools to the therapeutic arsenal. In our multivariate model, two pathological characteristics of the breast tumors were associated with phenotypic alterations: high histological grade and high Ki-67 expression.
This data strengthens the need to obtain corresponding information from patients in whom tumoral characteristics were associated with phenotypic alterations. These variables, namely, histologic grade 3 and high Ki-67 expression, which describe the capacities for differentiation and proliferation, may suggest the need to observe the pathological characteristics of nodal metastases, to effectively guide and optimize therapeutic strategies. The explanation for why these two pathological factors may influence the possibility of phenotypic alteration is based on the fact that undifferentiated tumors may show more intratumoral heterogeneity, wherein the population of cells that gain the characteristics of epithelial-tomesenchymal transition may differ from the principal types of cells observed in the originally analyzed samples. Therefore, a group of cells that are under-represented in the primary tumor may establish themselves by displaying metastatic capacity. The data obtained in this study is insufficient to confirm this theory; moreover, technical details of the experimental approaches may also contribute significantly to the resulting data.
In conclusion, the explanations for our data may range from the presence of technical issues or false negatives, to intratumoral heterogeneities, or to an actual alteration in the characteristics of the metastases observed in this study. Nevertheless, taken pragmatically, the selection of tumors with the abovementioned characteristics underscores the importance of the evaluation of the expressions of HRs and HER2 in different tissues, to appropriately tailor the individual therapeutic strategies.
Despite the fact that we do not know yet if this may offer further prognostic or predictive information [18], longer follow-ups and larger sample sizes may allow us to determine if the prognoses of patients may change as immunohistochemical information shift in metastatic development. Such a study will be presented in the future, when the required results are available.




 XML Download
XML Download