

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast metastases from extramammary malignancies are uncommon, as most metastatic breast tumors are from the contralateral breast [12]. Extrapulmonary metastases from primary osteosarcomas are also uncommon, with metastatic osteosarcoma to the breast being extremely rare. Although several cases of metastatic osteosarcoma to the breast have been reported in the literature [34,5,6], none of them have exhibited the imaging features of this rare form of metastasis. Herein, we report a case of metastatic osteosarcoma to the breast, focusing on imaging features seen using dedicated breast imaging modalities.
CASE REPORT
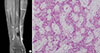
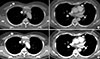
A 58-year-old Korean woman was referred to our institution for a mass in the right distal tibia detected with magnetic resonance imaging performed at an outside clinic (Figure 1A). The patient had been suffering from pain in her right ankle for a week. An open biopsy was performed, and the tumor was pathologically diagnosed as an osteoblastic conventional osteosarcoma (Figure 1B). She was transferred to our institution, where she subsequently underwent chest radiography and computed tomography (CT) for routine baseline evaluation. Although there was no evidence of pulmonary metastasis, two calcified nodules were discovered, one in the right breast and the other in the anterior mediastinum (Figure 2A). Based on imaging features, benign granuloma and metastasis were considered in the differential diagnosis, and short-term follow-up was recommended because the patient was scheduled for neoadjuvant intra-arterial chemotherapy. Chest CT performed three weeks later revealed size increases of the calcified masses (Figure 2B), raising the suspicion for metastasis. Therefore, the patient was referred to the breast radiologist for biopsy.
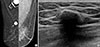
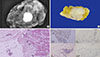
Diagnostic mammography (Figure 3A) showed a dense calcified mass in the right upper breast, with spiculated margins. Breast ultrasonography (US) of the right upper breast (Figure 3B) revealed a 1.5 cm dense calcified mass with posterior shadowing. Owing to the dense calcifications seen in the mass, percutaneous US-guided core needle biopsy was considered difficult to perform, and excisional biopsy was recommended to make a pathologic diagnosis. After the third cycle of neoadjuvant chemotherapy, excisional biopsies of the breast and mediastinal masses were performed. Specimen mammography (Figure 4A) of the excised breast mass showed the dense calcified mass within the specimen, confirming complete excision of the mass. Pathologic examination revealed a high-grade spindle cell tumor with osteoid matrix production (Figure 4B, C). Immunohistochemical staining revealed positivity for cluster of differentiation 99 (CD99) and negativity for estrogen receptor (ER), progesterone receptor (PR), and basal cytokeratins (CK5/6), which further suggested metastatic osteosarcoma to the breast (Figure 4D). The mediastinal mass was also excised via video-assisted thoracoscopic surgery, confirming metasta-tic osteosarcoma. Currently, the patient is being treated with adjuvant chemotherapy, with no clinical or radiological findings of recurrence after 2 months of follow-up.
DISCUSSION
Osteosarcoma is the most frequent skeletal malignancy and commonly involves the long bones of the extremities. Osteosarcoma most commonly metastasizes to the lung, followed by the skeleton, pleura, and heart [7]. In contrast, breast and soft tissues are extremely rare sites for metastatic osteosarcoma. The prognoses of metastatic patients remain poor even though the outcomes of patients with localized osteosarcoma have markedly improved due to the introduction of multiorgan chemotherapy. Extrapulmonary metastasis at initial diagnosis was an independent predictive factor of poor overall survival in a recent study [8].
Incidences of breast metastases from extra-mammary malignancies are reportedly very low. Most cases are incidentally found on CT during staging rather than on dedicated breast imaging (Table 1) [9]. The breast metastasis in our case was also initially detected by chest CT, as in another case recently reported by Chan et al. [5], in which the metastatic osteosarcoma appeared as multiple discrete, round nodules with dense calcification. In a case reported by Roebuck et al. [6], metastatic osteosarcoma to the breast was also seen by chest CT as a noncalcified, soft-tissue nodule in the right subareolar region. Another report included metastatic osteosarcoma to the breast detected on bone scan images, in which they exhibited intense tracer uptake at the chest wall outside the skeletal confinements. This was later proven to be a metastatic osteosarcoma [3]. Although a couple of case reports have presented mammographic features of primary breast osteosarcoma [1011], to the best of our knowledge, no studies have reported the mammographic findings of metastatic osteosarcoma to the breast.
In our case, the spiculated margins of the metastatic mass were well delineated on mammography, which strongly suggests malignant processes, including metastasis, rather than benign dense calcifications. On the other hand, US features of the lesion appeared relatively benign, as it was a well-circumscribed mass with dense calcifications. Mammography is more sensitive and accurate in evaluating breast calcifications, and as in our case, mammography may be more useful in differentiating between primary malignancies or metastases containing calcifications and benign calcified masses, such as involuting fibroadenomas. Additionally, as in our case, immunohistochemical staining helps to differentiate metastatic os-teosarcoma from other malignant breast lesions, such as metaplastic carcinoma with osteosarcomatous differentiation. CD99 is a commonly expressed osteosarcoma antigen [12], while ER and PR are well-known breast cancer biomarkers. Basal cell type cytokeratins, including CK5/6, are widely used for detecting myoepithelial differentiation, which is observed in sarcomatoid metaplastic carcinoma [13].
As there are no specific management guidelines for this extremely rare condition, metastatic osteosarcoma to the breast has been treated similarly to other metastatic masses. The general treatment strategy for osteosarcoma consists of local control by complete surgical excision and systemic chemotherapy. Complete surgical resection of all suspected metastatic lesions reportedly has survival benefits, and this is the only chance of a cure [14]. Both neoadjuvant and adjuvant chemotherapy are generally administrated before and after the surgery [14], but as of yet, there is no universal consensus on treatment of metastatic osteosarcoma to the breast [15].
In conclusion, although its incidence is very low, metastatic osteosarcoma should be considered when a dense calcified breast mass is found in a patient with a history of osteosarcoma. Dedicated breast imaging, such as mammography, is capable of providing clues to differentiate between metastatic osteosarcoma to the breast and benign calcified breast masses.

 XML Download
XML Download