

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Surgery is the most important treatment strategy for breast cancer. Breast-conserving therapy (BCT), consisting of breast conserving surgery followed by breast radiation therapy, has been considered on par with mastectomy as a standard surgical treatment once it was proven that the approach was not inferior in terms of survival outcomes compared with total mastectomy [12]. However, some breast cancers have multicentric or multifocal lesions in the ipsilateral breast [34], and these unexpected lesions may persist after breast-conserving surgery and cause locoregional recurrences [56]. Accordingly, surgeons need accurate preoperative imaging along with careful physical examinations to develop a precise surgical plan. Conventional preoperative imaging studies include mammography and breast ultrasonography. Recently, breast magnetic resonance imaging (MRI) has also been used for preoperative breast imaging [7].
The clinical role of preoperative MRI in patients with early breast cancer is controversial. Some investigators insist that preoperative MRI offers highly sensitive imaging that can help discover satellite lesions that cannot be detected with other conventional imaging methods [89]. Others argue that the low specificity of MRI leads to additional imaging with minimal benefit or an increase in the rates of unnecessary total mastectomy [1011]. In particular, recent studies suggest that preoperative MRI is not associated with reducing positive margins in patients who receive BCT [1213]. Furthermore, MRI imaging may lead clinicians to perform total mastectomies more frequently in patients with early breast cancer because of the detection of more subclinical satellite nodules that could be controlled by adjuvant radiation therapy [1415]. For this reason, those investigators suggested that preoperative MRI should be abandoned in routine practice for patients with early breast cancer. Several guidelines, including those from the National Comprehensive Cancer Network and the Korea Breast Cancer Society, specify that preoperative MRI can be used for specific clinical situations such as neoadjuvant settings and locally advanced breast cancer [1617].
To date, most studies regarding preoperative MRI have focused on the detection of additional cancerous lesions in the breast, and few studies have investigated clinical outcomes of preoperative breast MRI. We evaluated the effect of preoperative MRI on survival outcomes in patients with early breast cancer.
METHODS
Patient characteristics
We retrospectively reviewed the records of 1,025 patients between 2007 and 2010 who underwent definitive breast-conserving surgery for T1–2 breast cancer. Patients with inflammatory breast cancer, phyllodes tumor, Paget's disease, neoadjuvant chemotherapy, distant metastasis, or lack of radiation therapy after breast conserving surgery were excluded. Ultimately, 954 patients were included in the analysis and divided into two groups according to whether they received preoperative MRI or not. To compare the clinicopathologic features between the two groups, the following variables were analyzed: age, tumor size, nodal status, subtype, grade, estrogen receptor (ER) and progesterone receptor (PR) status, chemotherapy and radiation therapy status, and locoregional or systemic recurrence events. Approval for the study was granted by the Institutional Review Board of Yonsei University Hospital (number: 2015-0017).
Preoperative imaging technique
Preoperative MRI was performed with one of two types of a 3.0-T MR system (Intera Achieva, Philips Healthcare/Advanced Technology Laboratories, Bothell, USA; MAGNETOM Trio a Tim System, Siemens Healthcare, Erlangen, Germany) with dedicated, bilateral breast coils. The MRI protocol included a 3D coronal T1-weighted turbo fast low-angle shot sequence, transverse T2-weighted turbo spin-echo imaging, and dynamic contrast-enhanced MRI.
Histopathology
Tumor stage was based on the American Joint Committee on Cancer Staging manual sixth edition [18]. Histological grade was assessed by the modified Bloom-Richardson classification. ER and PR expression in the primary breast cancer were evaluated from formalin-fixed, paraffin-embedded whole sections of surgically resected breast cancer specimens using immunohistochemistry. Primary antibodies against ER (Clone SP1; Neomarkers for Lab Vision, Fremont, USA) and PR (Clone PgR 636; DAKO, Glostrup, Denmark) were used. The cutoff value for ER and PR positivity was greater than 10% staining by immunohistochemistry [19].
Treatment
Standard treatment for patients with breast cancer in our institution was described in a previous study [20]. In brief, along with breast surgery, sentinel lymph node biopsy or standard axillary lymph node dissection was performed in the BCT group. After definitive surgery, all patients received whole breast radiotherapy. Patients with hormone receptorpositive tumors received adjuvant endocrine therapy using selective estrogen receptor modulators or aromatase inhibitors. Most human epidermal growth factor receptor 2 positive tumors were not treated with adjuvant trastuzumab because the Korean National Health Insurance did not reimburse for trastuzumab before 2009.
Statistical analysis
We used Student t-test to compare mean values for continuous variables and results are given as mean±standard deviation. Pearson chi-square test and Fisher exact test were used for measuring statistical differences in categorical variables, and all statistical tests were two-sided.
Five-year locoregional recurrence-free survival (LRRFS), recurrence-free survival (RFS), and overall survival (OS) rates were calculated. LRRFS was calculated from the date of surgery to the date of locoregional recurrence. Locoregional or distant recurrence and death from any cause were considered RFS. The event of OS was death from any cause. The Kaplan-Meier method was used to plot survival and the log-rank test was applied to compare survival between groups. The Cox-proportional hazard model was used for both univariate and multivariate analyses. A p<0.05 was considered to be statistically significant. All statistical analyses were performed with SPSS Statistics version 20 (IBM Corp., Armonk, USA).
RESULTS
Of 954 patients who underwent BCT, 743 (77.8%) received preoperative MRI and 211 (22.2%) did not. The median follow-up time after surgery was 64.5 months (range, 1–100 months) for patients with preoperative MRI and 78.5 months (range, 0–101 months) for patients without preoperative MRI. The mean age was 48.9±9.06 years in the preoperative MRI group and 50.5±10.21 years in the conventional imaging group.
Clinicopathological characteristics of the two groups are summarized in Table 1. Patients younger than 50 years of age were more likely to undergo preoperative MRI than those older than 50 years of age (56.1% vs. 46.9%, p=0.018). More patients with preoperative MRI received hormonal therapy than did those without preoperative MRI (77.5% vs. 70.6%, p=0.034). Tumor size, nodal status, histologic type, grade, ER and PR status, and adjuvant chemotherapy were not significantly different between groups.
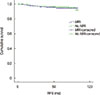
The log-rank test showed no significant difference between patients with preoperative MRI and those without in terms of LRRFS (p=0.938) (Figure 1), RFS (p=0.507) (Figure 2), and OS (p=0.655) (Figure 3). Univariate analyses for survival outcomes are summarized in Table 2. The tumor size (p=0.053) showed a marginal association with LRRFS. Tumor size (p<0.001), histologic grade (p=0.016), ER (p=0.015), PR (p=0.010), hormonal therapy (p=0.006), and adjuvant chemotherapy (p=0.031) were significantly associated with RFS. OS was significantly associated with tumor size (p=0.019), histologic grade (p=0.010), ER (p=0.010), PR (p=0.047), and hormonal therapy (p=0.014).
DISCUSSION
The detection of additional cancerous lesions via preoperative MRI is clinically valuable only if it improves outcomes such as tumor recurrence rate, re-excision rate, disease-free survival, and OS. Several studies have examined the accuracy of MRI, reporting a high sensitivity; however, other studies report its high sensitivity does not improve clinical outcomes [10212223]. Berg et al. [10] reported a retrospective analysis that included 121 cancerous breasts in which combined mammography, clinical examination, and MRI were more sensitive than any other individual test or combination of tests. Schnall et al. [21] also described a multicenter prospective study with 426 patients with confirmed breast cancer in which preoperative MRI detected 24.3% additional cancer foci with 72.8% accuracy. Similarly, Van Goethem et al. [22] reviewed 67 patients with dense breasts and a malignant breast tumor intended for conservative surgery and concluded that MRI was more accurate in assessing tumor extent and multifocality in patients with dense breasts. According to these results, the high sensitivity of MRI should lead to better survival outcomes in the preoperative MRI group, even if the tumors detected were clinically insignificant. However, Hlawatsch et al. [23] examined 104 women with findings highly suggestive of malignancy in the breast with mammography, sonography, and MRI before surgery and asserted that routine MRI was unnecessary, even though it is the most sensitive method for detection of small tumors, because of its meager clinical benefit.
Two prospective randomized trials, the Comparative Effectiveness of MRI in Breast Cancer (COMICE) and MR Mammography of Nonpalpable Breast Tumors (MONET) trials [2425], were performed to evaluate the effect of preoperative MRI on surgical outcomes. The COMICE trial reported no significant difference in re-operation rates between the study and control groups. The MONET trial reported a higher reexcision rate in the preoperative MRI group. Collectively, these prospective trials and retrospective studies focused on sensitivity and short-term surgical outcomes of preoperative MRI, and they did not describe any survival outcomes.
There are a few retrospective studies that set endpoints of survival outcomes, and the results have been inconsistent. Fischer et al. [26] compared 121 patients with preoperative MRI and 225 patients without and reported a decreased incidence of local recurrence 40 months after treatment in the MRI group. However, the cancer stage was less advanced in the MRI group and adjuvant treatment was not balanced between the groups. Another retrospective study reported that the use of breast MRI at the time of initial diagnosis was not associated with an improvement in outcomes after BCT even though clinicopathologic features of both patient groups were different [27]. Patients in the preoperative MRI group were younger and had smaller tumors. Recently, there was a study that matched study groups to overcome these limitations. Sung et al. [12] investigated the effect of preoperative MRI on surgical and long-term outcomes in breast cancer by comparing patients with and without MRI, matching the groups for age, tumor stage, and tumor histologic features. The investigators concluded that the use of preoperative MRI was not associated with a statistically significant improvement in long-term outcomes.
In our study, we compared patients with or without MRI during preoperative evaluation who received BCT. By virtue of our single institute design and the large number of included patients, preoperative MRI findings were systematically and uniformly linked to the operative plan and outcomes. Furthermore, because insurance assured preoperative MRI started in 2007, the latest data was collected over a short period that minimized adjuvant treatment bias. In the current study, clinicopathologic characteristics and adjuvant treatment status between the preoperative MRI and control groups were not significantly different, with the exception of age and hormonal therapy status (Table 1). In agreement with previous studies of long-term outcomes [12], our results showed that preoperative MRI did not affect survival outcomes in T1–2 breast cancer patients who received BCT. This result was supported by multivariate analyses in the current study. The reason that younger patients were more common in the preoperative MRI group was because younger patients are more likely to agree to MRI to evaluate the possibility of breast-conserving surgery before definitive surgery.
There are some limitations to this study. Because of recent advances in screening and multimodal treatment, survival outcomes of early breast cancer are excellent. There were relatively few events (total recurrence events, 43 of 954 [4.5%]; locoregional recurrence events, 11 of 954 [1.2%]; and death events, 22 of 954 [2.3%]). Because MRI for preoperative imaging was gradually introduced, the follow-up periods for both groups were not equivalent (median follow-up of MRI vs. control, 64.5 months vs. 78.5 months, respectively). Although the differences were minor, patient characteristics were not completely balanced. Patients older than 50 years of age and without hormone therapy were more prevalent in the non-MRI group. However, the multivariate analyses that were adjusted for these potentially confounding factors indicated that preoperative MRI was not associated with changes in survival outcomes.
Preoperative breast MRI has become more common in Korea recently because the national insurance system covers 90% of the cost of MRI and the cost to patients is only about 150,000 KRW in our institution. This subsidization allows easy access to preoperative MRI for patients and surgeons in Korea, even though controversy still exists regarding the use of preoperative MRI. In this setting, Korean doctors commonly choose MRI as a preoperative evaluation method. According to results of this study, however, preoperative MRI does not affect long-term survival outcomes. To confirm these results, a randomized, prospective clinical trial should be conducted.





 XML Download
XML Download