

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neoadjuvant chemotherapy (NAC) has several advantages over adjuvant chemotherapy in patients with breast cancer. For advanced stage breast cancer, NAC can, theoretically, decrease subclinical distant metastasis, and several studies have shown improvement in surgical options [123]. These benefits have changed the treatment regimens in breast cancer and have raised many questions concerning the factors that account for prognosis [4]. Before the NAC era, a number of variables including axillary lymph node metastasis, nodal ratio, tumor size, and tumor location were reported as prognostic variables for disease related survival. However, the implementation of NAC for breast cancer treatment has necessitated the re-evaluation of pre-existing prognostic factors; among these factors, a number of variables have been evaluated in the NAC setting and showed clinical significance. However, the prognostic role of tumor location has not been evaluated in breast cancer patients who underwent NAC. According to previous reports, in patients with breast cancer, a tumor in the inner/both quadrants has long been regarded as a worse prognostic factor for survival than a tumor in the outer quadrant [5678].
In the present study, we evaluated the prognostic significance of tumor location in breast cancer patients treated with NAC.
Go to : 
METHODS
Between March 2002 and January 2007, a total of 179 breast cancer patients who underwent NAC treatment were retrospectively analyzed. The eligibility criteria were breast cancer diagnosis pathologically confirmed via core needle biopsy; initial clinical stage II or III with lesions measurable by computed tomography (CT) and/or magnetic resonance imaging (MRI); normal bone marrow; and intact hepatic, cardiac, and renal functions. The NAC regimen consisted of docetaxel (75 or 60 mg/m2) and doxorubicin (60 or 50 mg/m2) by intravenous infusion every 3 weeks for three cycles. Subsequently, patients underwent curative surgery with either breast-conserving surgery (BCS) or modified radical mastectomy (MRM) with axillary lymph node dissection. Following the surgery, patients received three cycles of docetaxel and doxorubicin chemotherapy followed by radiation and/or hormonal therapy, if indicated. Radiotherapy (RT) was administered differently depending on the surgical method used. The patients who underwent BCS received a total dose of 50.4 Gy at 1.8 Gy per fraction with five fractions per week to the whole breast, followed by an electron boost of 10 Gy to the initial tumor bed. In patients who underwent mastectomy, the target volume included the chest wall and the regional lymph node area and the same dose schedule was applied. The patients who underwent mastectomy did not receive a boost to the tumor bed. RT was delivered to the internal mammary nodes (IMN) when they were clinically or pathologically involved. IMN RT was considered as a treatment option in multicentric tumors that were possibly aggressive. Adjuvant hormonal therapy was administered according to hormone receptor and menopausal status. Premenopausal women were treated with tamoxifen for 5 years, and postmenopausal woman were treated with an aromatase inhibitor or sequential tamoxifen followed by an aromatase inhibitor.
Examination of clinical and pathologic findings
We divided the patients into two groups according to the location of their tumors during the initial physical examination and according to CT and/or MRI images. The inner/both quadrant group included patients with tumors involving the upper/lower inner quadrant +/− multicentric tumor involving the outer quadrant, and the outer quadrant group included patients with tumors involving the upper/lower outer quadrant only.
In addition to tumor location, we evaluated the prognostic values of pathologic findings and treatment characteristics. Among the pathologic findings, we evaluated tumor size, lymph node status, nodal ratio, and estrogen receptor and/or progesterone receptor status. The cutoff value of nodal ratio was determined according to the result from a previous study conducted at our institution, which showed a difference between relapse-free survival and overall survival (OS) by a nodal ratio of 0.25 [9]. For analysis, pN0 was included in the group with a nodal ratio ≤0.25. Among the treatment characteristics, hormonal therapy and IMN RT were evaluated. Additionally, we evaluated initial clinical stage and pathologic complete response (pCR) including ductal carcinoma in situ. We defined pCR as no residual invasive tumor in the breast. Only tumors with residual intraductal carcinoma were included in the pCR group. This study protocol was reviewed and approved by the Institutional Review Board (H-1108-055-373).
Statistical analysis
The characteristics of the inner/both quadrant group and outer quadrant group were compared using the Pearson chi-square test. Local recurrence was defined as recurrence at the ipsilateral residual breast or chest wall. Regional recurrence was defined as ipsilateral axillary and/or supraclavicular and/or IMN recurrence. Distant metastases included contralateral breast recurrence and other distant organ metastases. Disease-free survival (DFS) was defined as the interval between the date of initial NAC and the date of any disease recurrence. OS was defined as the period from the date of NAC to the date of death. The Kaplan-Meier method was used for the assessment of disease-free, locoregional recurrence-free, distant metastasis-free, and overall survival. We used the log-rank test for univariate analysis in different patient groups. The variables identified by univariate analysis as statistically significant were included in the multivariate analysis using the Cox proportional hazards regression model. All p-values <0.05 were considered statistically significant. All statistical analyses were performed using the SPSS version 18.0 software (SPSS Inc., Chicago, USA).
Go to :
RESULTS
Treatment outcome
In the present study, 179 patients with a median age of 46 (28–69) years received NAC. Of these, 82 patients had outer quadrant tumors and 97 patients had inner/both quadrant tumors. Patients and treatment characteristics according to tumor location are summarized in Table 1.
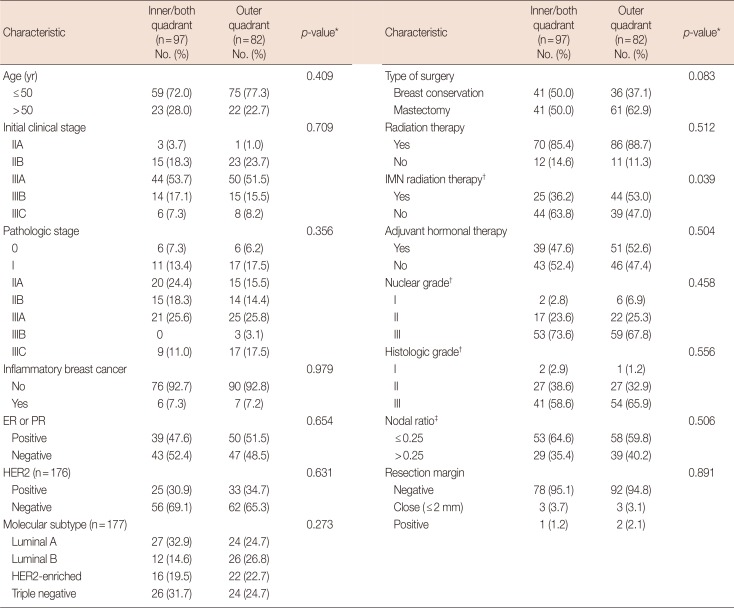
Table 1
Patients and treatment characteristics according to initial tumor site (n=179)
![]()
All patients received a total of six cycles of docetaxel and adriamycin chemotherapy, which was administered in two parts as three cycles before and three cycles after breast surgery. NAC did not cause any significant toxicity thereby circumventing any dose reduction or treatment delay. The median interval time from the last day of NAC to surgery was 25 (8–71) days. One hundred two patients underwent MRM and 77 patients underwent BCS. Positive or close resection margins were observed in nine patients (5.0%), and additional surgery was discouraged according to the institutional policy except in one patient who underwent additional total mastectomy owing to diffuse tumor infiltration. If indicated, adjuvant RT and hormonal therapy were offered. In total, 90 patients received adjuvant hormonal treatment and 156 patients underwent adjuvant RT. All patients who underwent RT after MRM received RT locally and to their chest walls. Among patients who underwent BCS, 34 patients (44.2%) received whole breast RT only, and 43 patients (55.8%) received regional RT in addition to whole breast RT. Majority of the patients who underwent MRM (65/79, 82.3%) and a small proportion of those who underwent BCS (4/77, 5.2%) received IMN RT (n=69).
The median follow-up duration was 61.1 (12–106) months. Fifteen patients (15/179, 8.3%) achieved pCR after NAC, and there was no regional lymph node metastasis (pN0) in 53 patients (29.6%). When the clinical stage before NAC was compared to pathological stage, 107 patients (59.8%) were down-staged while 38 patients (21.2%) had the same stage, and 34 (19.0%) had progressive disease. For all patients, the 5-year DFS, locoregional recurrence-free survival (LRRFS), distant metastasis-free survival (DMFS), and OS rates were 74.8%, 93.0%, 81.0%, and 89.9%, respectively.
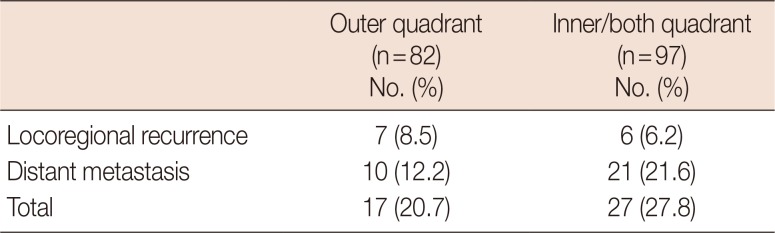
Pattern of failure
Total treatment failure was observed in 44 out of 179 patients (24.6%). According to the initial tumor location, the patient groups showed similar locoregional control rates (outer quadrant, 7/82, 8.5%; inner/both quadrant, 6/97, 6.2%) (Table 2). Distant metastasis was the major pattern of failure in both patient groups (21/27, 77.8%). Three contra-lateral breast recurrences occurred (outer quadrant, 2; inner quadrant, 1), which were regarded as distant metastases.
Univariate analysis
Pathologic stage (p<0.001), nodal ratio (p<0.001), and tumor location (p=0.020) were identified as prognostic factors for DFS (Figure 1A) whereas, the initial clinical stage (p= 0.049) and pathologic stage (p=0.034) were identified as prognostic factors for LRRFS (Table 3). DMFS correlates with pathologic stage (p<0.001), nodal ratio (p<0.001), and tumor location (p<0.004) (Figure 1B). The prognostic factors for OS were age (p=0.045), initial clinical stage (p=0.032), type of surgery (p=0.023), pathologic stage (p=0.006), nodal ratio (p<0.001), and hormonal therapy (p=0.010). Although tumor location was not a statistically significant factor for LRRFS and OS, patients with outer quadrant tumors showed better LRRFS and OS than those with inner/both quadrant tumors (Figure 1C and D). Although statistically insignificant, we observed that RT to the IMN improved LRRFS (95.5% vs. 91.4%; 5-year, p=0.265). pCR was not a statistically significant factor for LRRFS (p=0.924), DMFS (p=0.213), DFS (p=0.608), and OS (p=0.455).
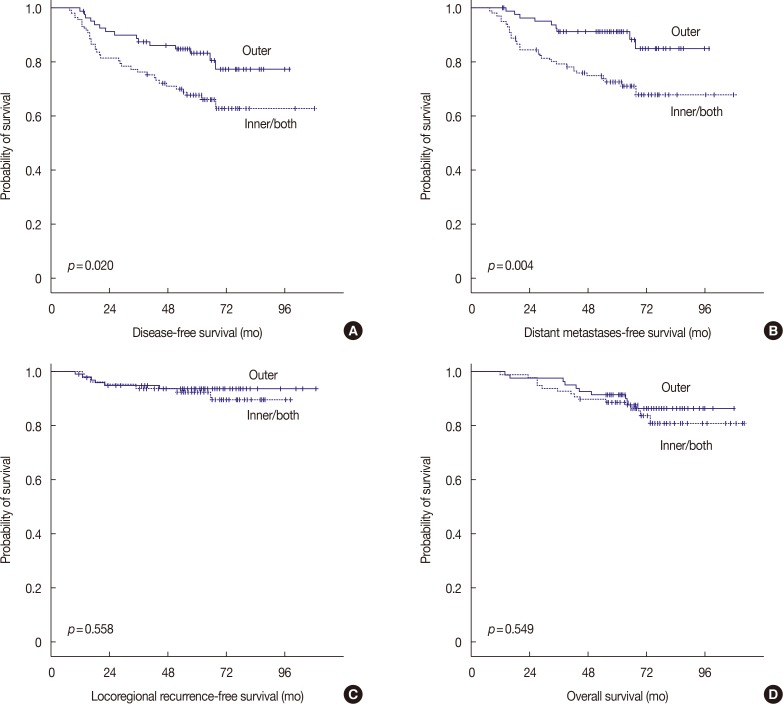 | Figure 1Survival curves according to tumor location. (A) Disease-free survival. (B) Distant metastases-free survival. (C) Locoregional recurrence-free survival. (D) Overall survival.
|
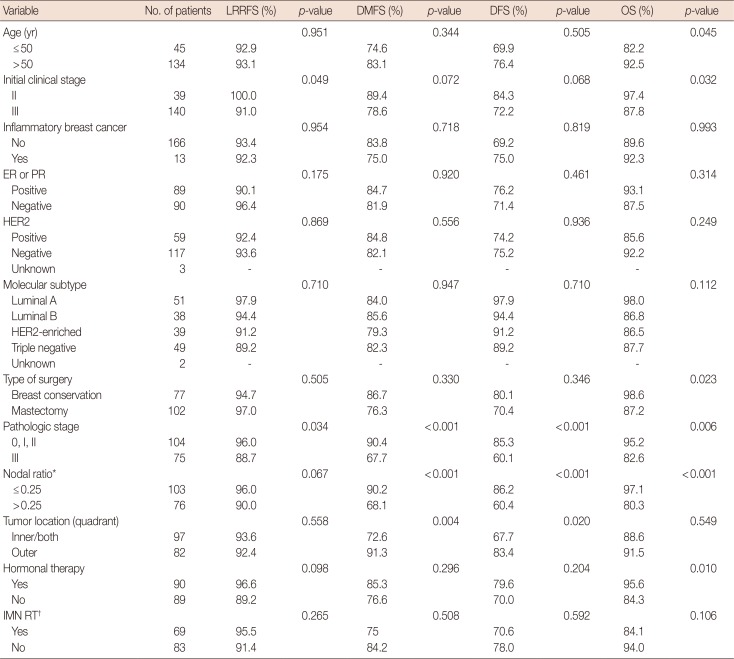
Table 3
Clinicopathological variables for 5-year disease-free, locoregional recurrence-free, distant metastasis-free and overall survival in univariate analysis (n=179)
LRRFS=locoregional recurrence-free survival; DMFS=distant metastasis-free survival; DFS=disease-free survival; OS=overall survival; ER=estrogen receptor; PR=progesterone receptor; HER2=human epidermal growth factor receptor 2; IMN=internal mammary node; RT=radiotherapy.
*Nodal ratio represents the ratio of the number of involved lymph nodes over the number of removed lymph nodes; †Available data (n=152).
![]()
Multivariate analysis
Using variables that were identified as statistically significant in univariate analysis, we performed multivariate analysis using the Cox proportional hazards regression model (Table 4). On multivariate analysis, pathological stage and tumor location were identified as independent prognostic factors for DMFS (p=0.001 and p=0.008, respectively) and DFS (p<0.001 and p=0.038, respectively). Nodal ratio and luminal A subtype were statistically significant factors for OS (p=0.002 and p=0.006, respectively). Multivariate analysis did not identify any statistically significant factors for LRRFS.
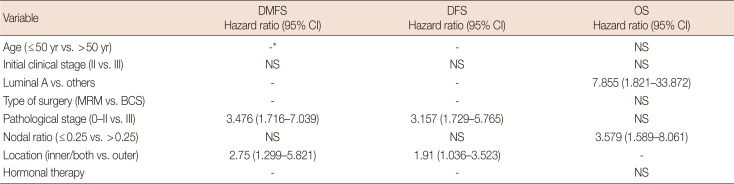
Table 4
Multivariate analysis of disease-free, distant metastasis-free, and overall survival
![]()
Go to :
DISCUSSION
The results of the present study suggest that despite three cycles of docetaxel and doxorubicin NAC for the treatment of breast cancer, patients with inner/both quadrant tumors showed unfavorable outcomes including DMFS and DFS compared to the outcomes in patients with outer quadrant tumors. To our knowledge, the present study is the first to show the effect of tumor location on survival outcomes of breast cancer patients who underwent NAC.
Previously reported studies using surveillance, epidemiology, and end-results data showed that tumors with inner quadrant locations had a negative effect on breast cancer-specific and OS rates [5]. In addition, according to several studies with respect to tumor location as a prognostic factor, inner quadrant tumors showed higher distant metastases and lower OS rates than those shown by outer quadrant tumors [678].
The reason of poor outcomes in patients with inner quadrant breast cancer is not clear; however, the idea that it might be related to IMN is generally accepted. The internal mammary basin is regarded as a second lymphatic drainage pathway and the incidence of IMN metastasis increases with the number of positive axillary lymph nodes in addition to tumor location [10111213]. These studies support the randomized phase III multicenter trial (EORTC 22922/10925), which evaluated the elective irradiation to the internal mammary and medial supraclavicular lymph nodes for potential survival benefit in node-positive or node-negative patients with central or medial tumors. IMN RT conferred a survival benefit in patients with inner or centrally located tumors [14]. Therefore, we secondarily sought to evaluate the effect of IMN RT. In the current study, more than half of the patients with inner/both quadrant tumors underwent IMN RT (44/86, 51.1%), which is higher than what was previously reported [915]. We did not have any institutional policy for the administration of IMN RT in patients with inner breast tumors; however, we included patients with multicentric tumors in the inner/both group and considered IMN RT for multicentric tumors, which might have influenced the high rate of IMN RT in the inner/both group. However, inner/both quadrant breast cancers maintained their worse prognosis despite the high rate of IMN RT. Furthermore, the IMN RT group failed to show a survival benefit compared to the non-IMN RT group among patients with inner/both quadrant breast cancer (data not shown). There are several possible explanations for these results. First, an incidental RT dose could have been delivered to the IMN in patients who did not receive IMN RT. In the dummy run of quality assurance study performed by the Korean Radiation Oncology Group, 59% of the prescribed dose was delivered to the IMN although physicians intended to exclude the IMN [16]. Secondly, most patients who received IMN RT underwent MRM (65/79, 82.3%), whereas a small portion underwent BCS (4/77, 5.2%). This skewed distribution and the interaction of treatment characteristics might have weakened the impact of IMN RT on the outcome.
Established prognostic factors for breast cancers should be re-evaluated in the NAC era. Regarding the molecular subtype and tumor location, Kim et al. [17] showed that triple-negative breast cancers had a tendency to develop close to the chest wall; however, there was a lack of data showing a correlation with inner quadrant breast cancers. Lim et al. [18] reported analyzed the data from 7,856 Korean women and reported that lower-inner quadrant tumors showed poor prognoses only in case of HER2 overexpression and triple-negative breast cancer. Some researchers have reported the prognostic value of nodal ratio after NAC, and have shown that this prognostic value is significant in certain molecular subtypes; however, the results are inconsistent [1920]. In the present study, we found that luminal A subtype breast cancer and a low nodal ratio conferred an OS advantage over the others; however, we could not identify any relationship between the molecular subtype and tumor location as well as nodal ratio.
There are several limitations to the present study. Despite the homogeneity of NAC regimen, the RT field was heterogeneous especially in the BCS group, because there is no consensus on the RT field after NAC and surgery. As reported by the American College of Surgeons Oncology Group (ACOSOG) Z1071, among the patients who underwent BCS, only 23.6% received axillary RT and 49.4% received supraclavicular RT. Moreover, only 52.2% of the patients received RT to the supraclavicular area in patients who had mastectomy without reconstruction [21]. In our data, all patients who underwent RT after mastectomy received RT to the axilla and supraclavicular area. As ACOSOG researchers commented in their report, the management of regional nodes in node-positive disease is complex and needs to be addressed in further randomized studies.
In addition, in the present study, the pCR rate (15/179, 8.3%) was lower than what was previously reported [22]. The optimal duration of NAC has not been established to date; therefore, we adopted three cycles of NAC. Reitsamer et al. [23] showed in 45 breast cancer patients that six cycles of epidoxorubicin/docetaxel prior to surgery had better pCR rates than three or four cycles of chemotherapy. In this perspective, our study might have inevitably showed a lower pCR rate than six cycles of chemotherapy [2324].
In conclusion, despite NAC, the inner/both quadrant tumor location as well as advanced pathological stage in breast cancer was associated with lower DMFS and DFS compared to those of outer quadrant tumor. For overcoming the unfavorable outcomes associated with inner quadrant involvement in breast cancer, as well as for better disease control and long-term survival, more aggressive neoadjuvant and/or adjuvant chemotherapy with IMN RT might be required.
Go to :
 XML Download
XML Download