

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the most common cancer, and is the leading cause of cancer death among women worldwide [1]. Despite the recent increasing incidence of breast cancer, the mortality due to the disease has been decreasing because of advanced treatment methods and early detection. Consequently, even patients who developed breast cancer can survive for longer periods and the requirements for breast cancer surgery have changed. In breast-conserving surgery (BCS) in particular, favorable cosmetic outcome has been defined as an important endpoint.
Although various evaluation methods have been reported, there are no defined criteria for a "favorable cosmetic outcome." Additionally, there are two methods used in cosmetic evaluation: the subjective method and objective method, respectively. Harris et al. initially proposed a 4-staged subjective evaluation method scored as "excellent," "good," "fair," "poor" in 1979 (Harris) [2,3,4,5]. In 1988, Aaronson et al. [6] reported a scoring method where a comprehensive evaluation was performed by scoring the subjective assessment. In Japan, the evaluation of postoperative cosmetic outcome by the Japanese Breast Cancer Society Sawai group (Sawai group) was proposed in 2004. In this scoring method, the evaluation was conducted using eight items related to the breast forms (breast size, breast shape, scar, breast firmness, nipple and areola size/shape, nipple and areola color tone, nipple position, and position of the maximum descent point of the breast) [7].
A desirable cosmetic evaluation method is an objective method that is independent of raters. As an objective method, Pezner et al. proposed the Breast Retraction Assessment (BRA) in 1985 [4,5,8]. In 2007, cosmetic evaluation methods utilizing photographic analysis software were proposed by two groups; the Breast Analyzing Tool (BAT), which was developed by Fitzal et al. [4,9,10,11], and the Breast Cancer Conservative Treatment cosmetic results (BCCT.core), which was developed by Cardoso et al. [3,4,5,10,12,13,14,15,16]. With high-quality images, the comparison between BAT and BCCT.core showed that BCCT.core, in which color assessment and scar assessment would also be carried out, showed a higher agreement rate to consensus [5,10]. In Europe, BCCT.core was used in a number of papers, and it was considered to be comparable to the several raters [3,5,17,18]. Nevertheless, the κ (weighted kappa; wκ) of BCCT.core compared to the consensus was 0.34 (0.53) and the agreement rate with the consensus was not necessarily high [10]. In addition, Asians including Japanese have smaller breasts than Caucasians, and therefore, inframammary fold is not as apparent in some cases. Since scars in Asians are more noticeable than in Caucasians, the BCCT.core, which had been developed based on the data in Europeans, was expected to affect the evaluation results. In this study, we compared and evaluated Harris (as a subjective evaluation), the Sawai group (as a subjective evaluation), and the BCCT.core (as an objective evaluation) to discuss the differences between the subjective and objective methods as well as address the issues that occurred when those methods were adapted to Asians including Japanese. Then we conducted observer assessment and examined the necessary elements for developing an ideal cosmetic evaluation method that is similar to subjective methods and is not influenced by raters.
METHODS
This study consisted of two parts: the primary evaluation and an observer assessment. In the primary evaluation, the head author himself compared and examined the Harris, the Sawai group, and the BCCT.core (developed and owned by Cardoso J, Cardoso M, and INESC Porto Breast Research Group) using the frontal photographs of breasts from 190 post-BCS cases. In the observer assessment, 100 out of 190 cases were selected so that the 4-staged scales (excellent/good/fair/poor) were distributed as equally as possible. Six raters compared the evaluations obtained by Harris and the modified Sawai group and considered the relationship between the elements, which constituted the cosmetic and 4-staged evaluations. Data were collected in accordance with guidelines for human subjects research, as approved by the Institutional Review Board of Mie University Hospital (2817) and Nakagami Hospital (2014025-2).
Photographs
Consent for photographs was obtained from the 190 patients. Photographs were taken with at least 7 mega pixels, in an examination room of approximately 10 m2 size, under ordinary fluorescent lights and a white background wall. The patient faced front with her chest thrust forward so that the outline of outer side of the breasts became apparent. When taking the photographs, we informed the patients that the photographs taken were to be used to compare the pre- and postoperational conditions of breasts and for research on cosmetic evaluation, and obtained their consents.
Primary evaluation
Methods of cosmetic evaluation
The Harris method [2,4] evaluated the overall impression using a 4-staged scale. An "excellent" rating means that the treated breast was nearly identical to the untreated breast. A "good" rating means that the treated breast was slightly different from the untreated breast. A "fair" rating means that the treated breast was not seriously distorted but clearly different from the untreated breast, while a "poor" rating means that treated breast was seriously distorted.
The Sawai group was a method that was initially proposed in 2004 and supported by the Japanese Breast Cancer Society [7]. It scores the following eight items and conducts evaluations with the highest total score of 12 points: breast size (0-2 points), breast shape (0-2 points), scar (0-2 points), breast firmness (0-2 points), nipple-areola complex (NAC) size/shape (0-1 point), NAC color tone (0-1 point), nipple position (0-1 point), and position of the maximum descent point of the breast (0-1 point). In this method, total scores of 11 to 12, 8 to 10, 5 to 7, and 0 to 4 points were defined as "excellent," "good," "fair," and "poor," respectively, indicating that the subjective evaluation results might be obtained pursuant to Harris. This is a subjective scoring method and identifies the elements that influence the cosmetic outcome. However, as it contains many evaluation items, is complicated, and is not easy to use.
In the BCCT.core [3,4,5,10,12,13,14,15,16,17] several objective evaluations were conducted for a comprehensive evaluation based on the measurement values of the computer software using frontal photographs of breasts. The software conducted cosmetic analysis by putting marks on the jugular notch and both nipples, and outlining the breasts with lines. The endpoints included the BRA, lower breast contour (LBC) [19,20], upward nipple retraction (UNR) [19,20], breast compliance evaluation (BCE) [21], breast contour length difference, breast area difference and breast overlap difference. In addition, the breast image was divided into 12 fractions by 30 degrees each. Color and scar assessments were conducted simultaneously for comparison between the left and right breasts. All the items were automatically conducted by the software. Eventually, 4-staged evaluation results may be obtained with results similar to that of Harris.
This assessment is based on frontal breast photographs, is easy to use, and is independent from raters. However, results are influenced by the conditions during the photo session (i.e., poses, lights). In addition, since it is a planar analysis of the frontal photograph of the breasts, three-dimensional (3D) forms may not be measured precisely.
Observer assessment
One hundred photographs out of 190 cases (approximately 25 cases each from four evaluation categories) were selected from the primary evaluation to ensure the equal distribution of cases in the 4-staged scale of evaluations scale. In each of the 25 cases, 15 cases had evaluation results by BCCT.core that were different from the two other methods, while the remaining 10 cases had evaluation results which were the same in all three methods. In cases with "poor" ratings, however, at least one of the all three methods were mainly selected because of the small number of cases. The evaluations were carried out by a total of six physicians: five expert breast surgeons who conduct BCS routinely and one plastic surgeon with experience in breast reconstruction. The six raters initially assessed the 100 cases according to the Harris method. Then, they evaluated the 100 cases using the modified Sawai group in order to determine the types of elements that are required for a cosmetic evaluation. Modified parts included the following seven items: breast size, breast shape, scar, NAC size/shape, NAC color tone, nipple position, and the position of the maximum descent point. Each item was scored between 0 to 5 points. In order to create a consensus for the raters with Harris as a whole, the first results was checked with a Delphi method, feedback was given and investigated. The relationship between the total consensus of the raters and the total scores of the seven items from the modified Sawai group was investigated using of a correlation coefficient.
Statistical analysis
During the primary evaluation, the degree of coincidence of the three evaluations methods were compared using the κ and wκ statistics in "IBM® SPSS® Statistics version 22 (IBM® Corp., Armonk, USA)". The degree of coincidence of κ and wκ is considered as follows: 0 as "poor," 0.01 to 0.20 as "slight," 0.21 to 0.40 as "fair," 0.41 to 0.60 as "moderate," 0.61 to 0.80 as "substantial," 0.81 to 0.99 as "almost perfect," and 1.00 as "perfect" [22]. In the observer assessment, the correlation was evaluated using Spearman rank-correlation coefficient. The relationships of values are shown as follows: <0.2 as "none," 0.2 to 0.4 as "weak", 0.4 to 0.7 as "moderate," and >0.7 as "strong."
RESULTS
Primary evaluation
Using the Harris method, 44 cases were evaluated as "excellent," 105 cases as "good," 24 cases as "fair," and 17 cases as "poor," respectively. In the Sawai group, 49 cases were evaluated as "excellent," 95 cases as "good," 29 cases as "fair," and 17 cases as "poor." In the BCCT.core, 31 cases were evaluated as "excellent," 102 cases as "good," 50 cases as "fair," and seven cases as "poor." Of these, 72 cases (37.9%) obtained the same results in the three evaluation methods while another three cases (1.6%) obtained three different results in all methods. For the level of coincidence, κ (wκ) was 0.096 (0.025) (slight) in the BCCT. core versus Harris, 0.128 (0.013) (slight) in the BCCT.core versus Sawai group, and 0.802 (0.796) (substantial) in the Harris versus Sawai group (Table 1), respectively. There is a significant difference between the BCCT.core as an objective evaluation and the Harris and Sawai group as subjective evaluations.
The photographs used in the primary evaluations were taken using heterogeneous backlight and background. Cardoso et al. [5,10] defined κ (wκ) in BCCT.core under such conditions as 0.43 (0.51). Based on this result, the degree of agreement rate of BCCT.core was inferior to the Harris and Sawai group.
For the details of each case, 13 cases were "excellent" or "good" in BCCT.core and "fair" or "poor" in other two methods. Cases shown in Figure 1A were "excellent" in BCCT.core and "fair" in other two methods. As such, the different evaluation results were considered to be caused by the lack of recognition of retraction due to scars in the 12 of 13 cases. On the other hand, 25 cases were "fair" or "poor" in BCCT.core and "excellent" or "good" in other two methods. Although the forms are equal in the right and left breasts (Figure 1B), measured values in BCCT.core were different due to the lack of volume, leading to "fair" or "poor" evaluation results in 15 cases. Some cases may be evaluated as "fair" depending on the degree of difference between the right and left breasts as shown in Figure 1C. However, even for the same "fair" cases, the definition of "fair" becomes different depending on the reason for the evaluation; due to retraction of the breasts, or lack of volume. There were also 10 cases for which evaluation results in BCCT.core were different at least two stages from that of the other two methods.
Observer assessment
In the consensus of whole raters obtained by the Delphi method, 27 cases were evaluated as "excellent," 27 cases as "good," 26 cases as "fair," and 20 cases as "poor." In the BCCT. core, 24 cases were evaluated as "excellent," 30 cases as "good," 39 cases as "fair," and seven cases as "poor." The degree of agreement between consensus and the BCCT.core was κ=0.134 (slight), showing low degree of agreement between the subjective methods and the BCCT.core. In particular, cases evaluated as "fair" and "poor" showed diverse evaluation results. Among cases evaluated as "fair" in the whole consensus, two cases were evaluated as "excellent" and five cases as "good" in the BCCT.core. Among cases evaluated as "poor" in the whole consensus, only one case was evaluated as "excellent" and four cases as "good" in BCCT.core.
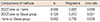
Scores rated by the six raters were calculated (30 scores in total) by items of the modified Sawai group, and the relationship between these scores and evaluation results obtained from the whole consensus (excellent/good/fair/poor) was shown in graphs (Figure 2). In addition, the correlation coefficient is shown as Spearman rank-correlation coefficient (Table 2). The shape of breasts showed the strongest correlation coefficient at 0.909 (Figure 2B), as indicated by the upwardsloping straight line in the figure. This was followed by the breast size 0.791 (Figure 2A) and the position of the maximum descent points 0.758 (Figure 2G). These items also showed upward-sloping lines in graphs of whole consensus (from "poor" to "excellent"), showing positive correlation. On the other hand, the scar showed the weakest correlation coefficient at 0.345 (Figure 2C), which means that it had almost no influence on the whole consensus. The line in the graph was also flat and showed that the scar had minimal influence on the evaluation results. Moderate correlation coefficient was observed in this order: nipple position, 0.690 (Figure 2F); nipple and areola size/shape, 0.647 (Figure 2D); and nipple and areola color tone, 0.542 (Figure 2E). The cosmetic evaluation is composed in order of breast shape>breast size>position of the maximum descent>nipple position>nipple and areola size/shape>nipple and areola color tone>scar.
DISCUSSION
Cosmetic outcome is an important element as well as a permanent cure for BCS. Although there are no defined criteria for cosmetic evaluation, the Harris evaluation method is one of the widely prevalent methods used for cosmetic evaluation of BCS in actual medical practice. A major concern for this method remains the differences caused by various raters. However, this can be resolved by using several raters for the same case. The BCCT.core uses software and is an objective method that not influenced by raters. In addition to integrated existing objective evaluation methods such as BRA, BCE, LBC, and UNR, employing color assessment in order to reflect the result of scar assessment and pigmentation secondary to radiation therapy is noteworthy. However, because of influences of photography conditions and limitations of color assessment, insufficient scar assessment is a concern.
As shown in the result of the primary evaluation, insufficient volume was noted in 15 out of 25 patients who were "fair" or "poor" in the BCCT.core but "excellent" or "good" in the other two methods. The reasons were as follows: (1) simultaneous breast cancer surgery for the affected breast and reduction mammoplasty for the nonaffected breast is not covered by national health insurance and is uncommon in Japan, and (2) the Japanese often resist surgery for the nonaffected breast (difference in the cultural backgrounds of Japan and Western countries). When assessed by BCCT.core, differences between the right and left breasts become significant because the assessment is conducted depending on the measurement values, leading to an assessment of "fair" or lower. In addition, the impact of the deterioration of cosmetic outcome due to the retraction of scars is different from that due to insufficient volume, but it is impossible to distinguish these assessment results. In the observer assessment also revealed that scar was not considered to be an important element on cosmetic evaluation. Breast-conserving therapy is a combination of BCS and irradiation of remaining breast. Since irradiation can make scar less noticeable to some extent, scars might be unregarded.
An ideal cosmetic evaluation method should not differ from a subjective one and should not be influenced by the raters. Close examination of the subjective assessment method and the development of a computer-based software to prevent differences among raters is essential. The agreement rates of BCCT. core and BAT to consensus were κ (wκ)=0.56 (0.64) and 0.39 (0.46), respectively, showing an unnecessarily high agreement rate to subjective evaluation [10]. This was because specific software conducted both the evaluations based on measured values in a large part. They did not integrate and reflect the forms that were based on subjective impressions or the balance of the relationship between breasts and other body parts.
The recent price reduction of 3D scanners may trigger their use in the development of a cosmetic evaluation [4,5,23]. Considering their convenience in a routine medical practice, however, 2D assessment with frontal photographs of breasts will continue.
In adapting the BCCT.core, an objective evaluation method, to Asian breasts, a clear difference between the objective and subjective methods was revealed. An ideal cosmetic evaluation method for BCS should be an objective method that is not far from the subjective method and is independent from raters. An examination of the elements that comprise a cosmetic evaluation, showed that those that related to breast configuration composed the most part of the evaluations. In a future study, we would like to continue the development of an ideal cosmetic evaluation method that is simple, similar to subjective evaluations and not influenced by raters.



 XML Download
XML Download