

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Fibroadenoma is a common benign breast lesion occurring in 25% of asymptomatic women [1]. Although previous studies of patients with fibroadenoma report an increased risk of breast carcinoma compared to similarly aged women in the general population, malignant transformation from fibroadenoma to cancer is rare [2]. Furthermore, Worsham et al. [3] reported that the presence of fibroadenoma, regardless of whether the lesion was proliferative or nonproliferative, was protective against breast cancer progression, a result that conflicted with the findings of previous studies. Therefore, management of fibroadenomas has typically been conservative [4]. Lesions that show typical features of fibroadenomas are classified as Breast Imaging Reporting and Data System (BI-RADS) category 3; if the lesion is considered to be involuting, it is classified as BI-RADS category 2.
In this article, we report a case of breast cancer that arose adjacent to or from an involuting fibroadenoma. There have been several case reports and studies that retrospectively reviewed breast cancers that arose within fibroadenomas; however, none of these studies reported serial changes in radiologic features of the cancer site, including findings from mammography and ultrasound (US). In this article, we report a case of breast cancer that arose adjacent to or within a fibroadenoma. Data from the case reported here include mammographic, sonographic, and magnetic resonance (MR) images that were also correlated with pathologic features.
CASE REPORT
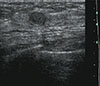
A 39-year-old woman with dense breast tissue underwent breast US as part of her regular screening exam at a local hospital. The US revealed a 0.7 cm nodule located in the upper-outer quadrant (UOQ) of her left breast, classified as BI-RADS category 3 (Figure 1). A follow-up US was recommended.
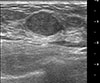
Two years later, the patient revisited our hospital complaining of a palpable mass in the UOQ of the left breast. US revealed a 1.8 cm circumscribed isoechoic mass in the UOQ of her left breast. It appeared that the previously noted nodule had increased in size (157% over 2 years), and the nodule was then classified as BI-RADS category 4A (Figure 2). This reclassification indicated a need for US-guided core biopsy, which confirmed that the nodule was a fibroadenoma. Subsequent surgery was recommended, but the patient refused and elected to undergo regular follow-up instead.
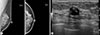
The patient returned to our hospital after 5 years, because she had been told during a routine follow-up exam performed at an outside hospital that calcifications had newly developed in the lesion. Her mammogram showed macrocalcifications that were centrally located within the lesion and that had a "popcorn-like" appearance (Figure 3A). US revealed that the nodule had decreased in size while also developing internal calcifications, findings indicative of an involuting fibroadenoma (Figure 3B). Because she was scheduled to undergo hormone replacement therapy for menopausal symptoms, the patient was concerned about the presence of calcifications. She wished to have a repeat biopsy of the lesion prior to initiating hormone replacement therapy. The rebiopsy confirmed the diagnosis of fibroadenoma, and the patient began hormonal therapy, which she continued for 3 years.
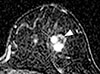
Another 4 years later, 11 years after the initial fibroadenoma diagnosis, the patient revisited our imaging center because the nodule had increased in size, according to an US result she had received from her local hospital. The patient underwent mammography at our hospital; this showed that the fibroadenoma was denser but the size of the lesion was similar compared to that of her previous exam (Figure 4A). We also performed US of the lesion, which revealed that the fibroadenoma had enlarged eccentrically and was accompanied by a 0.8×1.3 cm, microlobulated hypoechoic lesion. No changes in the previously detected calcifications in the UOQ were noted (Figure 4B). The lesion was classified as BI-RADS category 4A, and a core biopsy was indicated. The biopsy targeted the eccentrically enlarged portion, which was delineated on the US exam. Biopsy confirmed that the lesion was an invasive ductal carcinoma (IDC). For preoperative evaluation, MR imaging was performed and revealed a 1.5 cm enhancing mass in the UOQ of the patient's left breast, which correlated with the lesion detected on US (Figure 5).
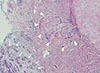
The patient underwent breast conservation surgery, which identified a 1.4 cm IDC (estrogen receptor 90% positive, progesterone receptor 60% positive, human epidermal growth factor receptor 2 negative) abutting the previously confirmed fibroadenoma (Figure 6) without axillary metastasis. She underwent postoperative definitive radiation therapy targeted to the left breast.
DISCUSSION
Fibroadenomas are common benign lesions of the breast that usually present as a single breast mass in young women [4]. There is some controversy regarding whether patients with fibroadenomas have an increased risk of subsequent breast cancer relative to other women. However, because malignant transformation from fibroadenoma is rarely reported, the management of fibroadenomas is typically conservative [4]. Complex fibroadenomas are a subtype of fibroadenoma that harbors one or more complex features, including epithelial calcifications, papillary apocrine metaplasias, sclerosing adenosis, or cysts larger than 3 mm [1]. The risk of developing breast cancer was found to be higher in patients with complex fibroadenomas than in those with noncomplex fibroadenomas (3.1 times greater among women with complex fibroadenomas versus 1.89 times greater among women with noncomplex fibroadenomas, compared to control groups) [5].
There have been some case reports of breast cancer arising within a fibroadenoma; however, these reports lack imaging findings in which the cancer is distinguishable from the fibroadenoma. Abe et al. [6] reported a case of scirrhous-type IDC arising in a fibroadenoma. On US, the suspicious palpable lesion appeared to have ill-defined heterogeneously hypoechoic features; however, the fibroadenoma and cancer components could not be distinguished. Monsefi et al. [7] reported a case of mucinous subtype IDC arising within a fibroadenoma with mammography images only. The lesion appeared to have a well-circumscribed border without calcifications, suggesting a benign lesion, most likely fibroadenoma. However, surgery revealed it to be a mucinous subtype of IDC [7]. Thus, it was difficult to find clues of cancers arising within or adjacent to fibroadenomas on imaging findings. More recently, Iwamoto et al. [8] reported a case of breast IDC that was adjacent to one of multiple macrocalcified fibroadenomas in a patient who had undergone mastectomy for the primary IDC more than 13 years earlier. The sonographic findings in Iwamoto et al.'s case report were similar to ours, particularly with regard to the hypoechoic mass with a microlobulated margin and microcalcifications adjacent to the macrocalcifications of the fibroadenoma. However, at the time of IDC diagnosis, the patient in Iwamoto et al.'s case already had axillary lymph node metastasis and had progressed far more than was the case with our patient.
Our case evaluation has some strengths that are distinguished from other published reports. First, we reported serial imaging findings of the fibroadenoma over time, which allowed us to demonstrate changes in the size of the lesion. During the follow-up, we could detect the newly developed malignant lesion adjacent to the fibroadenoma on the US images, based on regular screening mammography and US in a patient with heterogeneously dense breasts. We also correlated these findings with those of MR imaging performed during the preoperative evaluation. High-resolution ultrasonographic images enabled us to perform a targeted percutaneous biopsy of the suspicious lesion so that we were able to make the diagnosis of IDC before surgery, which is noteworthy because it meant we were able to diagnose IDC at an early stage (T1N0), without axillary lymph node metastasis.
Abe et al. [6] reviewed 15 cases of previously reported breast carcinomas occurring within fibroadenomas, among which carcinoma in situ was the dominant type (56.3%). They attributed this to the ability to make an earlier diagnosis of malignant neoplasm coexisting with an easily palpable fibroadenoma. However, in only two cases were these carcinomas <2 cm in size. In fact, the presence of fibroadenoma may obscure a small-sized cancer that is within or adjacent to the fibroadenoma if a meticulous evaluation is not undertaken. Therefore, it is encouraging that we were able to make a cancer diagnosis at an early stage based on regular screening mammography and US. However, we do not suggest that all involuting fibroadenomas require this type of follow-up. As many other previous case reports have suggested, even if the fibroadenoma is a benign neoplasm that is unlikely to undergo malignant transformation, radiologists should pay attention when imaging reveals newly developed suspicious features, such as irregular or microlobulated margins, increased size, or eccentric calcifications. Any changes that are newly detected should increase the concern for cancer.
In conclusion, we discuss the serial radiologic and pathologic findings of a case of breast cancer that arose adjacent to an involuting fibroadenoma. Fibroadenomas themselves and the malignancies arising within them can exhibit variable features on imaging studies. When new suspicious features are observed in a fibroadenoma, radiologists should raise the concern for breast cancer and proceed with diagnosis and treatment accordingly.

 XML Download
XML Download