

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The rate of breast cancer incidence has increased by approximately 33% over the past 30 years [1,2]. In patients with ocular metastasis, the primary tumor is generally diagnosed prior to ocular manifestation. The average interval between primary diagnosis and discovery of the metastatic lesion is generally 4.5 to 6.5 years, but delays of over 20 years have been reported [3]. Breast cancer generally metastasizes to the orbit via hematogenous spread and predominantly involves the choroid [4], whereas only a limited number of conjunctival breast cancer metastasis cases have been reported. To our knowledge, cases of subconjunctival breast cancer metastasis have not been previously described in the literature, so we present the first reported case of a metastatic subconjunctival mass associated with primary breast cancer.
CASE REPORT
A 41-year-old woman visited our clinic complaining of conjunctival injection and a foreign body sensation in the left eye, with no other systemic symptoms. She was treated with antibiotics and steroid eye solutions at a local eye hospital, and was later referred to our clinic because of disease progression. She had a history of breast cancer and had been treated 2 years previously with modified radical mastectomy followed by adjuvant radiotherapy (50.4 Gy, 28 cycles; 1,411.2 Gy in total) and six cycles of chemotherapy (cyclolphosphamide, methotrexate, and 5-fluorouracil). Pathological examination revealed an invasive ductal carcinoma (stage T2N1M0) that was moderately differentiated, negative for estrogen receptor/progesterone receptor expression, cytokeratin 5/6, and c-erb-B2, and positive for p53 (positive reaction in more than 51% of tumor cells) and Ki-67 expression (labeling index of 31% in tumor cells). Axillary lymph node metastasis was found in 1 out of 18 resected nodes.
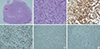
The best-corrected visual acuity was 20/20 in the right eye and 16/20 in the left eye, with an intraocular pressure of 9 mm Hg and 7 mm Hg in the right and left eyes, respectively. A slit lamp bi-microscopic examination showed a cystic mass under the temporal bulbar conjunctiva, associated with dilated overlying conjunctival vessels (Figure 1). The anterior chamber, lens, and media were clear, no signs of choroid or retina involvement were observed, and extraocular muscle movement was not limited. Informed consent was obtained from the patient before the surgery. An excisional biopsy revealed a poorly differentiated adenocarcinoma positive for carcinoembryonic antigen and p53, and negative for gross cystic disease fluid protein 15, thyroid transcription factor-1, and estrogen receptor (Figure 2). Positron emission tomography examination for systemic malignancy revealed multiple bony metastasis with bone marrow infiltration, multiple muscular and subcutaneous metastasis, multiple lung metastasis with metastatic subcarinal and left hilar lymph nodes, mesenteric metastasis, and pancreatic metastasis.
DISCUSSION
Metastasis to the eye develop most commonly from cancer of the breast (40%) and the lung (29%) [5]. Freedman and Folk [6] reviewed the charts of 112 patients (141 eyes) who presented with metastasis to the eye or orbit and revealed that breast cancer was the most common primary tumor (49.1%). Approximately 5.8% to 9.2% of visually asymptomatic patients with advanced or metastatic breast cancer develop ocular metastasis, which typically develop 2 to 5 years after the primary tumor has been detected [7,8,9]. In our case, an ocular metastasis was found 2 years after the primary tumor was detected.
The subconjunctival space is a potential space between the conjunctiva and sclera that does not normally contain blood vessels. Further, unlike the well-vascularized conjunctiva, the scleral stroma mostly consists of bundles of collagen fibers, occasionally accompanied by blood vessels and fibroblasts. As breast cancer metastasizes via the bloodstream, ocular metastasis tend to be located preferentially in the posterior uvea [10]. Metastatic subconjunctival masses are therefore very rare and, consequently, they can be easily mischaracterized as benign masses that are independent of the breast cancer. Although the precise mechanism is unclear, a sclera stromal blood vessel might have played a role in the metastasis case reported here.
Cancer metastasis to the eye are associated with a poor clinical prognosis, regardless of the type of primary cancer, with an average survival rate of only 15 months [6,11]. When breast cancer metastasizes to the eye, the risk of it spreading to the brain or central nervous system increases significantly. Although many patients die due to systemic disease, up to half of the patients die due to intracranial progression. The prognosis of patients with brain metastasis is poor, with a median survival time of 1 to 2 months in untreated patients and 3 to 6 months in patients treated with radiotherapy [12]. If the metastasis is detected early, metastatic lesions can be treated successfully with modalities such as external beam radiotherapy, radioactive plaque brachytherapy, and immunotherapy [13]. Although our patient did not have brain metastasis, the treatment time was delayed due to a late diagnosis. Therefore, metastatic disease should be considered in the differential diagnosis of subconjunctival lesions, and ophthalmic manifestations can play an important role in the detection of metastatic spread of a known primary breast cancer.

 XML Download
XML Download