

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Human epidermal growth factor receptor 2 (HER2) is overexpressed in approximately 15% to 25% of breast cancers. Structurally, HER2 is comprised of three parts: a transmembrane domain, an extracellular domain, and an intracellular tyrosine kinase domain. The extracellular domain may be cleaved and shed from the surface of the tumor cell by tissue metalloproteinases at the juxtamembrane region of HER2, at which point there is a measurable increase in the level of serum HER2 extracellular domain (serum HER2) in the blood [1]. This increase in serum HER2 is associated with poor prognosis and HER2-targeted treatment resistance in patients with HER2-positive metastatic breast cancer [2,3,4,5]. In 2003, the U.S. Food and Drug Administration approved the measurement of serum HER2 by the ADVIA Centaur® immunoassay analyzer (Siemens Medical Solutions Diagnostics, Tarrytown, USA) as a specific method for monitoring trastuzumab treatment in metastatic HER2-positive breast cancer patients.
Despite the obvious clinical value of serum HER2 measurement in monitoring disease status in metastatic patients, the clinical utility of serum HER2 measurement for the detection of disease recurrence in postoperative breast cancer patients has not yet been established. Since the overexpression of HER2 in primary tumors is associated with a poor prognosis, early detection of disease recurrence using simple methods, such as the identification of blood tumor markers, would be extremely beneficial in clinical practice. The most widely used blood tumor markers for the detection of breast cancer recurrence are carcinoembryonic antigen (CEA), carcinoma antigen 15-3 (CA 15-3), or a combination of both [6]. However, the routine use of CA 15-3 or CEA for monitoring disease recurrence in patients after primary breast cancer treatment is not recommended by the American Society of Clinical Oncology [7]. The application of serum HER2 for the early detection of breast cancer recurrence has not been extensively investigated, and it may offer an alternative to the currently available methods. To date, few studies discuss the clinical value of serum HER2 as a tumor marker for the detection of disease recurrence; most of these studies analyzed serum HER2 levels in patients with metastatic disease, and only a small number of patients with HER2-positive disease were evaluated [8,9]. In theory, serum HER2 levels cannot increase without the existence of a HER2-positive tumor. Therefore, the purpose of this study was to investigate the validity and importance of the measurement of serial serum HER2 levels for the detection of disease recurrence in HER2-positive breast cancer patients who have undergone curative surgical resection of their primary tumor and are under long-term follow-up care.
Go to : 
METHODS
Study patients
Serial serum HER2 levels were measured in patients with invasive ductal or lobular HER2-positive breast cancer who had undergone curative surgical treatment between January 2008 and December 2010. HER2 positivity was detected using immunohistochemistry (IHC), and HER2 amplification was measured using fluorescence in situ hybridization (FISH); the set IHC rating and FISH ratio for defining HER2 positivity was 3+ and >2.2, respectively. Other clinicopathological variables such as age at diagnosis, disease stage, hormone receptor status of the primary tumor, and disease recurrence were obtained from the Korea Cancer Center Hospital Breast Cancer Database. Tumor stage was classified according to the American Joint Committee on Cancer, 7th edition. During blood sample collection for serum tumor marker assessment, information on serum aspartate aminotransferase (AST) levels, alanine aminotransferase (ALT) levels, and the history of liver disease was obtained from a chart review. Disease recurrence, including locoregional recurrence and distant metastasis, was confirmed by a biopsy of the metastatic lesion or by imaging methods (computed tomography, ultrasound, mammography, magnetic resonance, bone scanning, and/or positron emission tomography-computed tomography). Serum HER2, CEA, and CA 15-3 levels were measured at baseline and at the time of regular outpatient follow-up after surgery. This study was approved by Korea Cancer Center Hospital Institutional Review Board (K-1308-002-002).
Serum HER2, CEA, and CA 15-3 measurements
The ADVIA Centaur® automated immunoassay analyzer was used to analyze serum HER2 levels. This automated chemiluminescence immunoassay system measures circulating levels of the extracellular domain of the HER2 oncoprotein by using two monoclonal antibodies raised to two distinct epitopes of serum HER2. Previous studies report a cutoff of 15.2 ng/mL for serum HER2 [10,11]. We validated this cutoff value in our laboratory, and any serum HER2 level above the cutoff value was considered to be elevated. Serum CEA and CA 15-3 levels were measured using a Modular Analytics E170 analyzer (Roche Diagnostics, Naka, Japan), and their cutoff values were 4.6 ng/mL and 25 U/mL, respectively, based on the manufacturer's instructions.
Statistical analyses
All statistical analyses were performed using SPSS for Windows version 14.0 (SPSS Inc., Chicago, USA). Receiver operating characteristic (ROC) curves were drawn and the area under the curve (AUC) was calculated for each marker. The sensitivity of serum HER2, CEA, and CA 15-3 was calculated according to a previous study [12]. The association between serum HER2 and serum AST/ALT levels was assessed using the Pearson correlation coefficient (r). A p-value of less than 0.05 was considered statistically significant.
Go to :
RESULTS
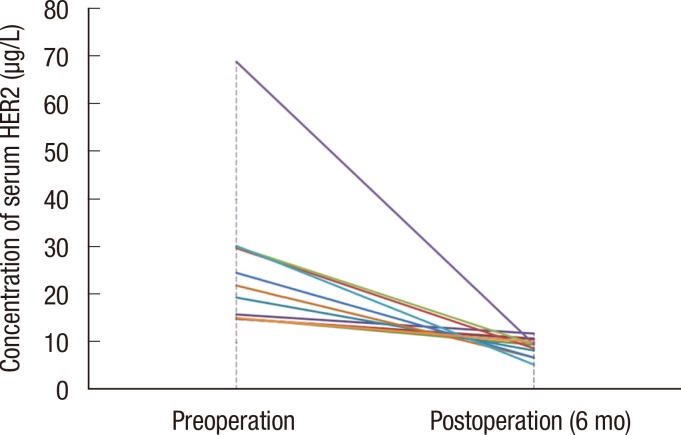
Overall, 264 patients were eligible for this study. The mean age at the time of surgical treatment was 50.9 years, and the median follow-up period was 27.7 months. Table 1 shows the characteristics of the study population. Of these 264 patients, 12 showed elevated serum HER2 levels at the time of first diagnosis. After 6 months, and after curative surgical resection of the primary tumor, the serum HER2 level of all patients was restored to within normal levels (Figure 1). Four patients who showed elevated serum HER2 levels at the time of first diagnosis subsequently suffered disease relapse. Of these four patients, two patients also showed increased serum HER2 levels at the point when disease recurrence was detected. In the patients with elevated serum HER2 levels at the time of first diagnosis and without disease recurrence, serum HER2 levels remained within the normal range over the entire course of follow-up.
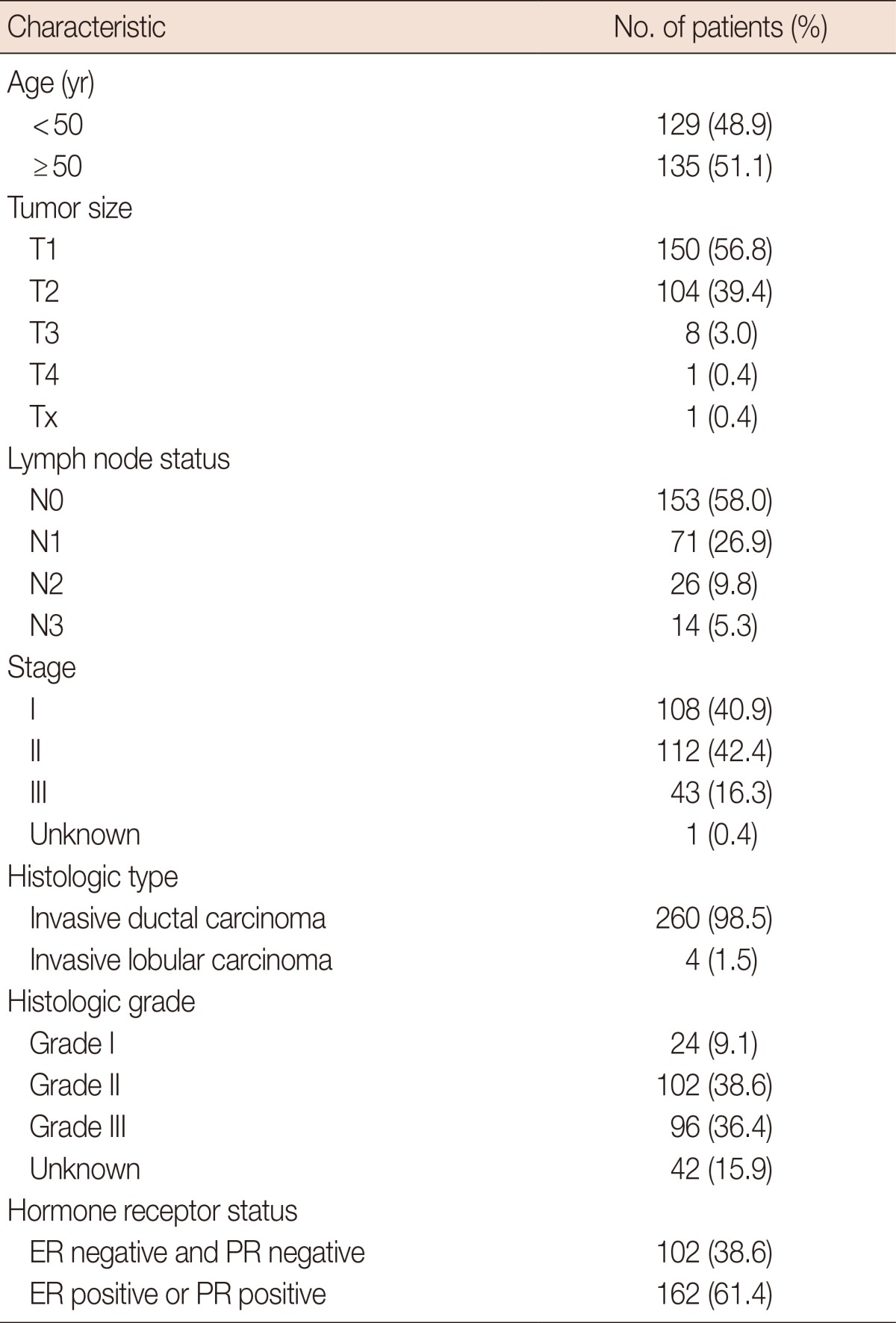
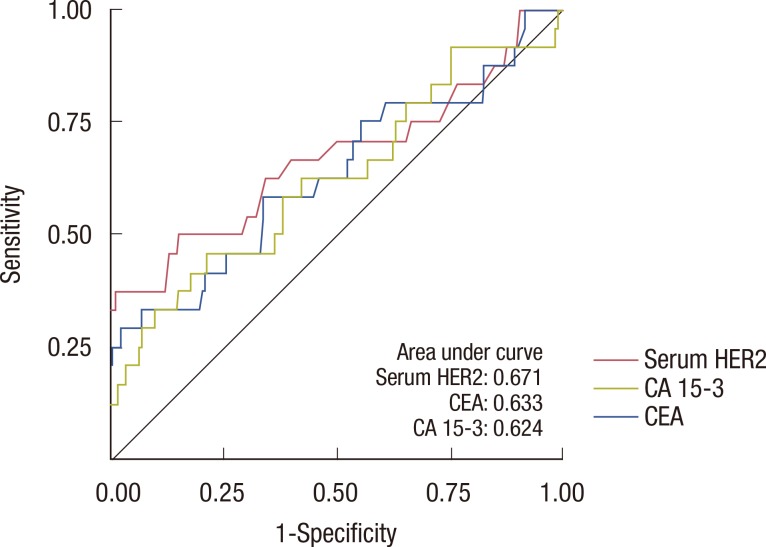
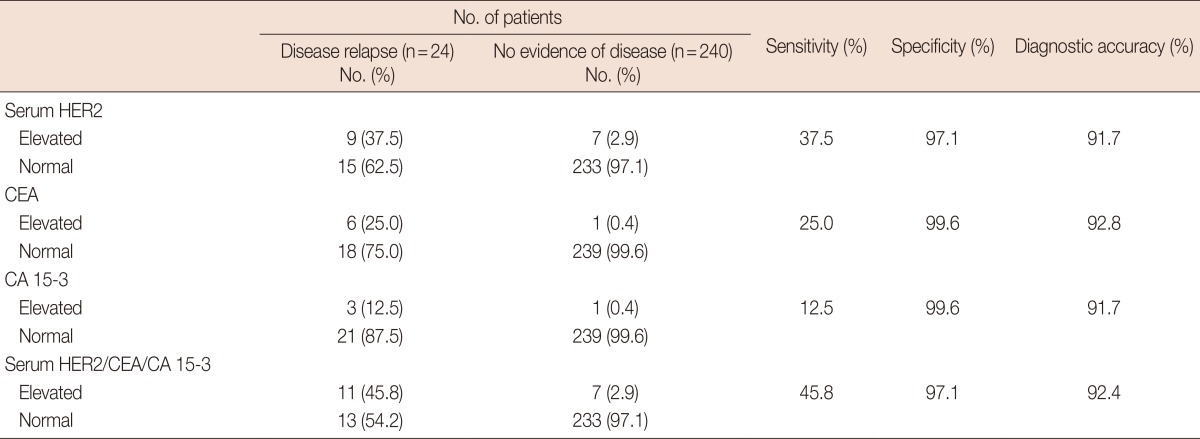
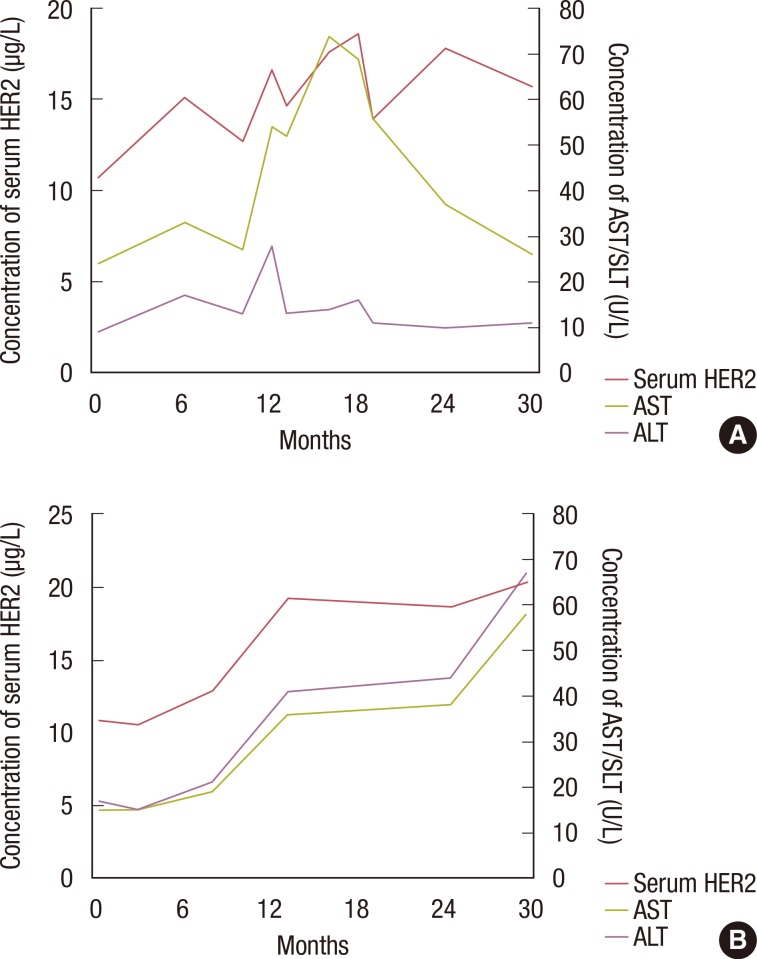
Twenty-four patients demonstrated disease recurrence during the follow-up period. Of these patients, four developed local or regional recurrence and 20 developed distant metastases. At the time of disease recurrence, the serum HER2 levels of nine patients were higher than the defined cutoff value (Figure 2), one of whom suffered local recurrence and one demonstrated regional recurrence. Distant metastasis was found in the remaining seven patients. The sensitivity for detecting disease recurrence using serum HER2, CEA, and CA 15-3 levels was 37.5%, 25.0%, and 12.5%, respectively (Table 2). Based on the ROC curve, the AUC of serum HER2 (0.671) was greater than that of CEA (0.633) and CA 15-3 (0.624) (Figure 3). After combining all three tumor markers, the sensitivity improved to 45.8%.
 | Figure 2Changes in serum human epidermal growth factor receptor 2 (HER2) levels in patients with disease recurrence at follow-up. (A) Case I. A 26 years woman presented lung metastasis at 16 months after curative operation. At the time of disease relapse, elevated serum HER2 was observed. (B) Case II. A 54 year woman showed liver metastasis at 18 months after breast conservative surgery. Elevated serum HER2 level was checked at the time of diagnosis of disease relapse.
|
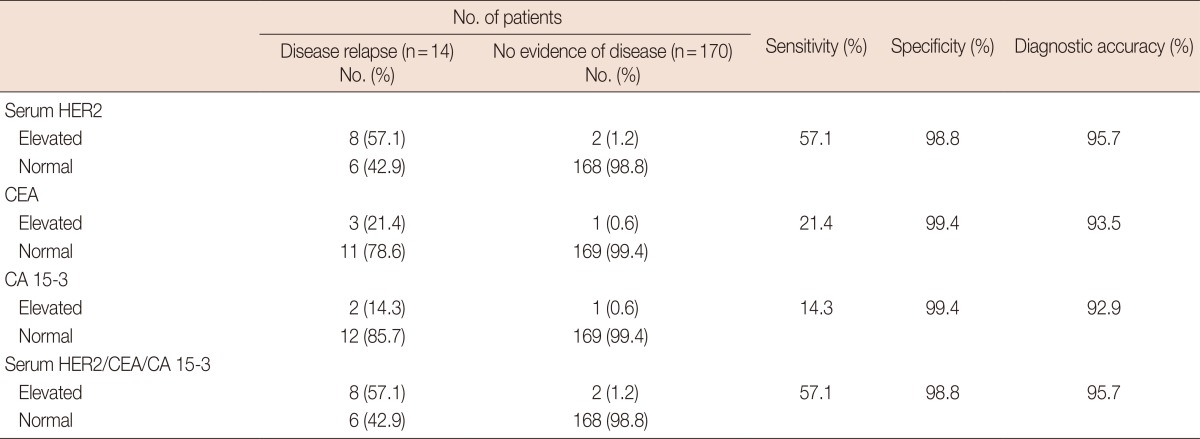
Given that serum HER2 levels can be influenced by liver disease, we reviewed the relationship between abnormal AST or ALT levels and serum HER2. In some patients, an association was found between serum HER2 levels and the levels of AST/ALT (Figure 4). We evaluated the relationship between serum HER2 level and AST/ALT level in 863 samples from the 223 patients with no evidence of metastasis during the postoperative follow-up period. Serum HER2 levels were significantly associated with AST levels (r=0.344, p<0.001) (Figure 5) and ALT levels (r=0.254, p<0.001) measured concurrently. Of the 264 patients, 80 had abnormal AST or ALT levels during the follow-up, chronic hepatitis, or liver cirrhosis. After excluding these patients, the sensitivity of serum HER2 for the detection of disease recurrence increased to 57.1% (Table 3). In the ROC curve, the AUC of serum HER2 (0.781) was greater than that of CEA (0.650) and CA 15-3 (0.677) (Figure 6).
 | Figure 4Changes in serum human epidermal growth factor receptor 2 (HER2), aspartate aminotransferase (AST), and alanine aminotransferase (ALT) levels in patients with elevated serum HER2 levels and no evidence of disease recurrence. (A)Case I. A 47 year patient presented mild fatty liver during the follow up period. The serum HER2, AST, ALT level has been changed simultaneously. During the follow up period, there was no evidence of disease recurrence. (B) Case II. A 45 year patient without any past history of liver disease showed elevated serum AST/ALT level. The serum HER2 level showed similar movement with the fluctuation of serum AST/ALT level. There was no evidence of disease relapse during follow up period.
|
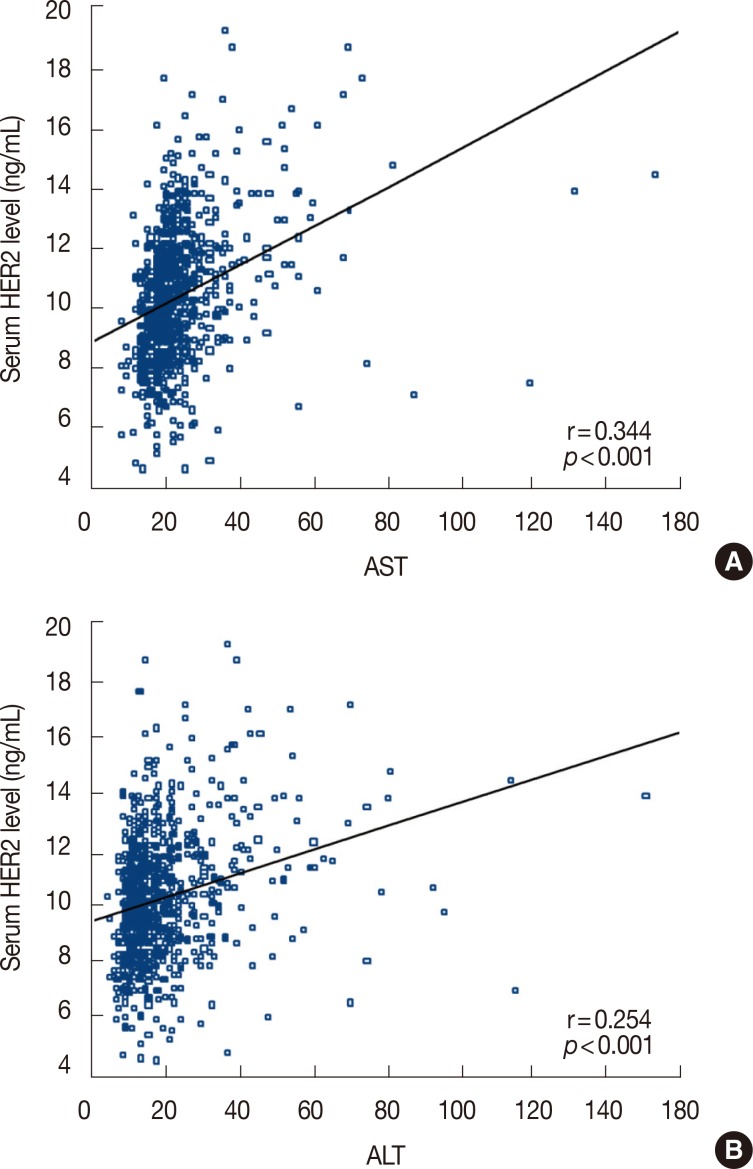 | Figure 5The relationship between serum human epidermal growth factor receptor 2 (HER2) and serum aspartate aminotransferase (AST) (A) and alanine aminotransferase (ALT) (B).
|
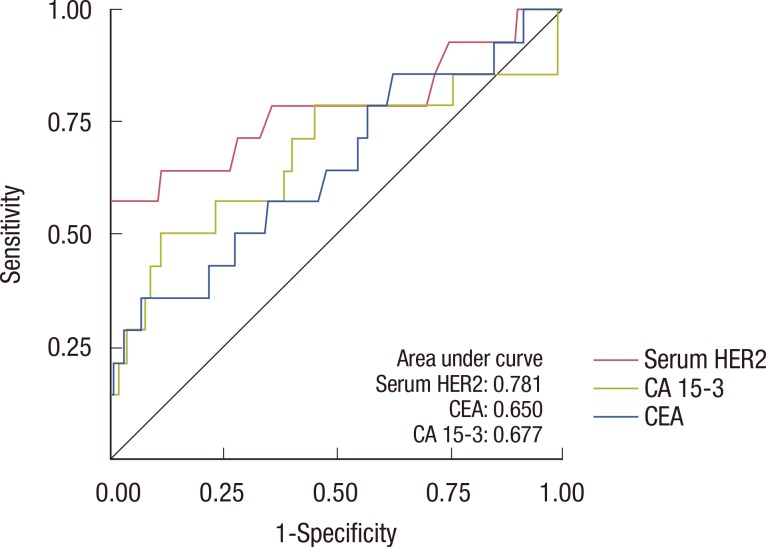 | Figure 6Receiver operating characteristic (ROC) curve for serum human epidermal growth factor receptor 2 (HER2), carcinoembryonic antigen (CEA), and carcinoma antigen 15-3 (CA 15-3) levels in patients with normal aspartate aminotransferase (AST) or alanine aminotransferase (ALT) levels, chronic hepatitis, or liver cirrhosis.
|
Go to :
DISCUSSION
In this study, the sensitivity and specificity of serum HER2 for detecting disease recurrence in early breast cancer patients following primary treatment were similar to those achieved using CEA and CA 15-3. Furthermore, our results indicate that serum HER2 levels could be associated with mildly abnormal liver function. To the best of our knowledge, this is the first study to report that high AST or ALT levels correlate with falsely-positive serum HER2 levels for the detection of disease recurrence in breast cancer patients under regular surveillance following curative surgical treatment.
In 2003, the use of the ADVIA Centaur® immunoassay analyzer to measure serum HER2 was approved by the U.S. Food and Drug Administration as a step towards the monitoring of trastuzumab treatment in patients with HER2-positive metastatic breast cancer. However, the role of serum HER2 in the follow-up of breast cancer patients after curative surgical therapy has not been adequately investigated. In this longitudinal study, patients had undergone curative surgical resection of their primary HER2-positive breast cancer. We found that in some patients with recurrence detected at follow-up, the serum HER2 levels were higher than the defined cutoff value. The sensitivity of HER2 for detecting disease recurrence was 37.5%, but this increased to 45.8% when it was combined with CEA and CA 15-3.
Of the currently validated surveillance tumor markers for breast cancer, CEA and CA 15-3 are the most frequently used and most valuable markers for the diagnosis and monitoring of recurrence [13]. In the current study, we have shown that the sensitivity of serum HER2 was greater than that of CEA or CA 15-3 for detecting breast cancer recurrence. These results indicate that serum HER2 levels may be a more reliable tumor marker for evaluating disease recurrence during follow-up for HER2-positive breast cancer patients after curative surgical treatment. Few studies have probed the sensitivity of serum HER2 levels as a primary indication of disease recurrence for HER2-positive breast cancer and compared it to the sensitivity of CEA or CA 15-3. Pedersen et al. [14] investigated the sensitivity of CA 15-3, CEA, and HER2 for the early diagnosis of metastatic breast cancer. They showed that in a subgroup of 27 patients with a HER2-positive primary tumor, the sensitivity of HER2, CEA, and CA 15-3 were 55.6%, 51.9%, and 37.0%, respectively. Sugano et al. [15] performed a retrospective analysis of 158 patients during postoperative follow-up and found that the sensitivity of serum HER2 for detecting relapsed disease was 84.6% (11/13). Molina et al. [16] performed serial serum HER2, CEA, and CA 15-3 measurements in a cohort of 250 patients with primary breast cancer and found no evidence of residual disease after surgery. They also reported that serum HER2 sensitivity for early diagnosis was 83.3% (10/12). These studies employed a different cutoff value, and therefore, are not directly comparable to our study. However, they are in agreement with our results despite the variety of test assay methods and their small sample sizes. In fact, in all of the above studies, serum HER2 was found to be the best single tumor marker for the detection of disease recurrence in patients with HER2-positive primary breast cancer.
There is limited information regarding nonmalignant conditions that could lead to an increase in serum HER2. Molina et al. [17] investigated the serum HER2 levels in patients with benign disease. The study included 40 patients with benign breast diseases, 26 with liver cirrhosis, 14 with renal failure, 16 with benign lung disease, 6 with lupus, 5 with peptic ulcer, and 4 patients with other benign diseases. Abnormal serum HER2 levels were found in 38.5% of patients with liver cirrhosis (10/26 patients). Other patients with benign disease did not have serum HER2 levels >15 U/mL. Motoo et al. [18] evaluated serum HER2 levels in patients with digestive disease. At their cutoff value of 17 U/mL, 63.3% of patients with liver cirrhosis, 43.2% of those with chronic hepatitis, 42.9% of those with acute hepatitis, and 42.8% of those with other liver diseases had HER2 positive serum. The manufacturer's instructions recommend careful interpretation of these results in patients with bilirubinemia. However, in our study cohort, there were no patients with bilirubinemia. Since serum AST and ALT levels were positively associated with serum HER2 levels, we analyzed the sensitivity of serum HER2 after the exclusion of patients with abnormal AST/ALT levels without metastasis. The sensitivity of serum HER2 increased to 57.1% following the exclusion of all patients demonstrating high AST or ALT, chronic hepatitis, or liver cirrhosis.
This study has certain limitations, one of which is the short follow-up period. The median follow-up period was 27.7 months, and events occurred in 24 patients (9.1%). Although the sensitivity of serum HER2 for detecting disease recurrence in this study was 37.5%, long-term follow-up may be necessary to further evaluate the true value of serum HER2 as a tumor marker in early breast cancer patients. In addition, although there was a significant association between serum HER2 and serum AST/ALT levels, this finding is difficult to translate to clinical practice because the increase in AST/ALT was mild, and there was no accompanying bilirubinemia. Taken together, these limitations, along with the high cost of serum HER2 measurement, may restrict the application of serum HER2 measurements for clinical applications.
In conclusion, the measurement of serial serum HER2 levels might be a possible method for the detection of disease recurrence in carefully selected HER2-positive breast cancer patients. Elevated serum HER2 levels should be interpreted carefully in patients with high serum AST or ALT levels, as this is associated with a high false positive rate. Although the results of this study indicate that the exclusion of patients with high AST levels, high ALT levels, or chronic liver disease could improve the sensitivity and specificity when measuring serum HER2 levels, there is only a small increase in the sensitivity and specificity values for CEA and CA 15-3 levels. Physicians should, therefore, take into account that the measurement of CEA and CA 15-3 is not recommended for routine surveillance of breast cancer patients after primary therapy, as specified in globally accepted guidelines, including those of the American Society of Clinical Oncology [7]. However, prospective randomized trials could be helpful to validate the use of routine surveillance of serum HER2 in HER2-positive breast cancer patients after primary treatment.
Go to :
 XML Download
XML Download