

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Microglandular adenosis (MGA) is a rare benign disease that causes proliferative glandular lesions in the breast. These benign lesions may progress to a wide spectrum of disease, from atypical microglandular adenosis (AMGA) to carcinoma arising in microglandular adenosis (CAMGA). Although MGA itself is benign, it can cause carcinoma, which can lead to problems if not excised completely. In this study, we report two cases of invasive carcinoma arising in MGA.
CASE REPORTS
Case 1
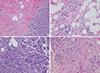
Case 1 was a 44-year-old woman with a previous history of breast-conserving surgery because of ductal carcinoma in situ (DCIS) in her right breast 4 years ago. After breast-conserving surgery, she received radiotherapy on her right breast but no hormonal therapy or chemotherapy. During a regular follow-up, ultrasound examination revealed an abnormal nodular lesion in her left breast. She had no symptoms or signs associated with a breast mass. On physical examination, no palpable mass was found in either breast. Mammography showed heterogeneously dense breast tissue and a newly developed small nodular density at the left upper outer quadrant of the breast (Figure 1A). Ultrasound examination revealed an ill-defined irregular hypoechoic nodule measuring approximately 8 mm and an ill-defined hypoechoic nodule measuring approximately 7 mm (BI-RADS category 4b) at the 1 to 2 o'clock region and 5 cm from the left nipple. Both nodules were adjoining (Figure 1B). Ultrasound guided localization excisional biopsy and frozen section revealed that the lesion was invasive carcinoma. She underwent modified radical mastectomy (MRM) with sentinel lymph node biopsy (SLNB). No definite mass-like lesion was found on gross examination (Figure 2). Microscopic examination revealed widely spread round proliferative glands lined by a single layer of flat to cuboidal epithelial cells and lacking a myoepithelial layer, indicating typical MGA. In part of the lesion, the glandular lumen was obliterated by proliferation of monotonous, atypical small cells with frequent mitotic figures, indicating carcinoma in situ. A cord-like arrangement and irregular aggregates of highly atypical cells were scattered in the stroma and extended into the adipose tissue (Figure 3). Immunohistochemical (IHC) staining revealed the following: S-100 protein (+), estrogen receptor (ER) (-), progesterone receptor (PR) (+, Allred score 3), human epidermal growth factor receptor 2 (HER2) (-), lysozyme (+), α1-antitrpysin (+), calponin (-), and p63 (-). The SLNB showed no evidence of metastasis. The final diagnosis was multifocal invasive carcinoma associated with DCIS (grade 3) arising in MGA with stage 1A, T1 (<1 cm, in the largest one), N0 (0/1), M0, and lymphovascular invasion (-). After surgery, she received adjuvant chemotherapy and hormonal therapy. After 14 months of medical follow-up, no evidence of recurrence has been found.
Case 2
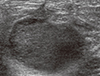
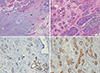
Case 2 was a 57-year-old woman with a palpable mass in her right breast. No other symptoms were associated with the mass. On physical examination, a firm, movable mass measuring approximately 3 cm was palpable at the right upper outer quadrant of the breast. Nipple retraction was observed. She had no medical or familial history of cancer. Mammography revealed a huge mass-like lesion at the right upper breast and ultrasound revealed a lobulating heterogeneous hypoechoic mass measuring 2.6×2.2 cm at the 11 o'clock region of the right breast (Figure 4). Positron emission tomography revealed fluorodeoxyglucose (FDG) uptake at a 2.7 cm hypermetabolic mass in the upper outer quadrant of the right breast (SUVmax: 15.4) and FDG uptake in lymph nodes of the right axilla (level 1). A core needle biopsy of the lesion suggested invasive carcinoma and encapsulated papillary carcinoma. The patient underwent right MRM with SLNB. A well-demarcated solid mass measuring 2.8×2.4 cm was found on gross examination (Figure 5). Microscopic examination revealed encapsulated papillary carcinoma arising in MGA, which exhibited atypia and variable proliferation (approximately 5.2 cm in the largest dimension). Most areas of the MGA were atypical and were lined by large pleomorphic cells with nuclear hyperchromasia and prominent nucleoli. A 0.3×0.25 cm focus of invasion was associated with an altered chondromyxoid stroma adjacent to the encapsulated papillary carcinoma. Typical MGA tubules with intraluminal colloid-like secretory material were found at the more peripheral area of the lesion (Figure 6). IHC staining revealed the followings: S-100 protein (+), smooth muscle myosin-heavy chain (-), ER (-), and PR (-). No metastasis was observed in the sentinel lymph nodes. The final diagnosis was invasive ductal carcinoma (grade 2) associated with encapsulated papillary carcinoma arising in MGA with stage IA, T1 (0.3×0.25 cm), N0 (0/5), M0, and lymphovascular invasion (-). The patient showed no evidence of recurrence on medical follow-up at 19 months. We consulted Dr. Fattaneh Tavassoli, a breast pathologist at the Yale School of Medicine, USA, about these two cases.
DISCUSSION
Since MGA was first described in 1968, by McDivitt et al. [1], several studies have reported cases of AMGA and CAMGA [2-7]. Both carcinoma in situ and invasive carcinoma can occur in MGA. In Korea, DCIS arising in MGA was reported by Jeong et al. [8]. To the best of our knowledge, the present cases are the first cases of invasive carcinoma arising in MGA to be reported in Korea. No more than 27% of carcinomas have arisen in MGA [2,6]. Although one report suggested that the incidence of carcinoma could be as high as 64%, it appears to have been affected by bias [9]. Results of IHC staining of carcinoma arising in MGA did not differ significantly from those of MGA. In most cases, results of IHC staining showed positivity for cytokeratin, E-cadherin, and S-100 and negatively for ER, PR, HER2, cystic disease fluid protein (GCDFP)-15, epithelial membrane antigen, smooth muscle actin, CD10, calponin, and p63. α1-Antitrypsin, cathepsin D, and lysozyme may also stain positively in some cases [5]. One of the major differences in IHC staining of MGA from invasive carcinoma is that MGA stains basement membranes with laminin and collagen IV. In MGA and carcinoma in situ, in contrast to invasive carcinoma, basement membranes are preserved. In the two cases presented here, the preliminary pathologic diagnosis was acinic cell carcinoma (ACCA), and it was revised to CAMGA after consultation with Dr. Tavassoli. In some cases, CAMGA is often misdiagnosed as ACCA if MGA goes unrecognized [10,11]. Some CAMGA cells are immunoreactive for amylase, lysozyme, and α1-antichymotrypsin, which are found in ACCA, indicating acinic cell differentiation [10]. In addition to this, both exhibit glandular structures and granularity as well as stain positively for S-100 and antitrypsin, and negatively for ER and PR [5,6]. The biopsy of one of our patients stained positively for lysozyme and α1-antichymotrypsin. Therefore, looking for underlying MGA is essential to making the definite diagnosis. Signs of MGA include regular nuclei, a single layer of cuboidal cells, basal lamina, eosinophilic luminal content, and empty cytoplasm on electron microscopy. In addition, MGA are negative for epithelial membrane antigen and GCDFP-15 in IHC staining. However, ACCA does not show regular nuclei and basal lamina, but shows granular cytoplasm and dense core granules on electron microscopy. It may or may not reveal a single layer of cells, cuboidal cells, luminal content, and GCDFP-15 in IHC staining [4,5,12].
Treatment of CAMGA should be individualized to each patient's stage of disease. If MGA is accompanied by AMGA or CAMGA, it must be completely excised with a negative surgical margin. Incomplete excision of a primary benign MGA lesion can cause recurrence of MGA with development of carcinoma [3]. It is difficult to secure a safety margin because of the insidiously invasive character of MGA, and cases of axillary lymph node metastasis and distant metastasis have been reported [13]. In addition to surgery, radiation therapy should be considered in patients with breast-conserving surgery, and adjuvant chemotherapy should be considered in patients with axillary metastasis or with invasive tumors larger than 1 cm in the absence of nodal metastasis [14]. Despite histopathological and IHC features indicating poor prognoses, most studies have reported relatively favorable prognoses [3,6,7,14,15]. However, longer follow-up periods are needed to determine the exact prognosis of CAMGA.



 XML Download
XML Download