

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the second most common cancer among women in Korea. Approximately 14,000 new cases of breast cancer occur each year in Korea and an estimated 240,000 occur each year in the United States. Most breast cancers are invasive ductal carcinomas (IDC), 'not otherwise specified' (NOS), and medullary breast carcinoma (MBC) is a rare histological type of breast cancer, accounting for 1% to 7% of all breast cancers [1-4].
In 1945, Moore and Foote described MBC as a unique histological subtype, characterized by high-grade structure with heavy lymphocytic infiltration, sharp circumscription, hemorrhagic necrosis, and a relatively favorable prognosis [5,6]. Some researchers, however, have questioned the prognosis and morphologic definition of MBC. Ridolfi et al. [7] reassessed MBC and documented strict criteria for diagnosing typical and atypical MBC. Diagnostic criteria for typical MBC include a predominantly syncytial growth pattern in more than 75% of the tumor area, circumscription with a pushing margin, moderate to marked lymphoplasmacytic infiltration, poorly differentiated nuclear grade with a high mitotic rate, scant stroma, and absence of an intraductal component. Atypical MBC differs from typical MBC in terms of pathologic features with an infiltrative margin, mild mononuclear infiltration, a low nuclear grade, and presence of an intraductal component [8].
Many previous studies have indicated that this histological type is associated with a favorable prognosis despite the presence of aggressive features such as large tumor size, a high nuclear grade, and hormone receptor (HR) negativity, which are usually accepted as poor prognostic factors [3,9,10]. The prognosis of MBC is still under dispute. Some studies have reported that MBC survival rates do not differ from those of IDC [11-13]. The clinicopathologic features of MBC have various implications that dictate not only diagnosis but also therapeutic approaches. The aim of this study was to compare the clinicopathologic characteristics of MBC with those of IDC and to clarify the prognosis of patients with MBC.
METHODS
We retrospectively reviewed the medical records of patients with invasive breast cancer who were surgically managed at the Breast Cancer Center of Samsung Medical Center, Seoul, Korea from August 1995 to June 2010. Patients with distant metastasis at diagnosis, those with ductal carcinoma in situ, or patients who received neoadjuvant chemotherapy were excluded. We also excluded patients with occult breast cancer presenting with axillary node metastasis, and patients with a history of ipsilateral or contralateral breast cancer.
In this study, MBC was defined according to the strict criteria of Ridolfi et al. [7], and only typical MBC was diagnosed as MBC. In our institution, atypical MBC is classified as IDC (NOS) in accordance with the literature indicating that the clinical course of atypical MBC is similar to that of IDC [14,15]. A total of 52 patients with MBC and 5,716 patients with IDC were included in this study. The authors retrospectively reviewed clinicopathologic features including tumor size; lymph node (LN) metastasis; pathologic stage; nuclear and histological grade with immunohistochemical findings, such as estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) status; treatment modalities (operation, adjuvant chemotherapy, radiotherapy, and hormone therapy); and recurrence or survival status.
Tumor stage was assessed according to the American Joint Committee on Cancer (AJCC) 7th staging system [16]. The histological grade was determined according to the Bloom-Richardson classification [17]. The Allred score system (range from 0 to 8) was used to evaluate ER and PR status, and a total score of >2 was defined as positive. An HER2 score of 3+ or 2+ with gene amplification determined by fluorescence/silver in situ hybridization was considered positive. Disease-free survival (DFS) was defined as no local or systemic recurrence and no newly developed contralateral breast cancer. The DFS and overall survival (OS) of patients with MBC were compared with those of patients with IDC.
This study was approved by the Institutional Review Board of Samsung Medical Center (SMC 2013-07-090).
Statistical analysis
Statistical analyses were performed using PASW statistics 18 software (SPSS Inc., Chicago, USA). Student t-test and the chi-square test (or Fisher exact test when appropriate) were used to compare the clinicopathologic characteristics of the MBC and IDC groups. The Kaplan-Meier method was used to determine DFS and OS rates, and survival curves were compared using log-rank tests. Multivariate analysis was performed using Cox proportional hazards model to yield the relative hazards of multiple variables, including histological type, on breast cancer recurrence or death. All p-values are two-tailed, and a p-value of <0.05 was considered statistically significant.
RESULTS
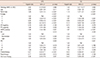
A total of 7,848 patients with primary invasive breast cancer were treated surgically at our institution during the study period. Among them, 6,828 patients (87.0%) were diagnosed with IDC-NOS, and 52 patients (0.7%) had MBC. A total of 5,716 IDC-NOS cases and 52 MBC cases met the eligibility criteria and were included in this study. The median follow-up periods were 53.5 months (range, 0.3-182.8 months) for IDC and 88.6 months (range, 0.9-194.6 months) for MBC. MBC patients were younger than IDC patients (mean age at diagnosis±standard deviation 44±9 vs. 48±10, p=0.005) (Table 1). All surgeries were classified as mastectomy or breast-conserving surgery (BCS), regardless of axillary node dissection. There was no significant difference in the operative method (p=0.341). More women in the MBC group were premenopausal (IDC 64.9% vs. MBC 74.5%, p=0.280).
The mean MBC tumor size was 2.25±1.47 cm and was not different from the mean IDC tumor size (2.37±1.21 cm, p=0.536). All MBCs manifested as a single lesion, whereas 16.9% of IDC had multiple foci (p<0.001). Interestingly, MBC had distinct features, such as no lymphovascular invasion (LVI) (IDC 27.8% vs. MBC 0.0%, p<0.001) and rare LN metastasis (N0 IDC 58.4% vs. MBC 86.5%, p<0.001). The average numbers of metastatic LNs were 0.2 in the MBC group and 1.9 in the IDC group (p<0.001). The MBC group had a significantly higher proportion of patients with a poor histological grade (grade III IDC 38.3% vs. MBC 80.0%, p=0.003) and higher nuclear grade (high grade IDC 41.7% vs. MBC 82.8%, p<0.001) as well as negative ER (IDC 31.0% vs. MBC 84.8%, p<0.001) and PR (IDC 38.8% vs. MBC 91.3%, p<0.001) statuses which are generally regarded as poor prognostic factors of invasive breast cancer. HER2 status did not differ significantly between the two histological groups (IDC 28.9% vs. MBC 37.5%, p=0.293). When patients were categorized according to molecular subtype, the MBC group predominantly had HR-/HER2+ tumors or triple-negative breast cancer (p<0.001).
There was no difference in the rates of chemotherapy between groups. More patients with IDC received hormone therapy than did patients with MBC (IDC 72.8% vs. MBC 12.0%, p<0.001) owing to HR status.
Kaplan-Meier curves showed that IDC and MBC had similar DFS and OS rates (5-year DFS 88.0% vs. 89.2%, p=0.920; 5-year OS 93.4% vs. 94.4%, p=0.503) (Figures 1 and 2). We compared DFS and OS between histological subtypes of same the pathologic stage categorized according to the 7th AJCC staging system, and found that survival did not differ according to histological subtype (DFS: stage I, p=0.193, stage II, p=0.853; OS: stage I, p=0.684, stage II, p=0.815). As shown in Table 2, when the prognosis of the two histological groups were compared, no differences in recurrence or death due to disease were observed in subgroup analysis of nodal status, HR status, HER2 status, and adjuvant treatment although this differed on subgroup analysis for node-positive disease and use of hormone therapy. On survival analysis for each molecular subtype of IDC and MBC, the DFS and OS of MBC were the closest to the outcome of Luminal A type (HR+/HER2-) of IDC; however, this finding was not statistically significant (Figure 3).
We performed multivariate analysis of the entire population using a Cox proportional hazards model to identify the effect of histological subtype on recurrence or death, after adjusting for already known prognostic factors including age, tumor size, lymph node metastasis, HR/HER2 status, LVI, nuclear grade, histological grade, chemotherapy, and hormone therapy. Radiotherapy (p=0.013) and relatively advanced age (p=0.011) improved DFS but were not associated with OS. When adjusting for other factors, the DFS and OS associated with medullary histology itself was not significantly different from those associated with IDC (DFS: hazard ratio 0.85, 95% confidence interval 0.12-6.05, p=0.866; OS: hazard ratio 1.49, 95% confidence interval 0.21-10.77, p=0.692) (Table 3).
To identify the prognostic factors specific to MBC, a univariate survival analysis was performed for known prognostic factors using the Kaplan-Meier method with the log-rank test. We did not identify differences in DFS or OS in MBC patients according to tumor size, HR status, HER2 status, or adjuvant treatment. However, the survival curve for patients with LN metastasis differed significantly from that of patients without LN metastasis (DFS, p=0.010; OS, p<0.001) (Figure 4). The prognosis of patients with MBC seemed to be determined by known prognostic factors, such as nodal status, rather than the histological type itself. As shown in Table 4, all MBCs associated with LN metastasis presented as HR-negative tumors with a high nuclear grade. Distant recurrence with or without locoregional recurrence occurred in three of these patients.
DISCUSSION
This retrospective review of invasive breast cancer at a single institution in Korea helped elucidate the clinicopathologic characteristics of MBC. In this study, MBC had several specific features. However, prognosis of MBC did not differ from that of IDC and was determined by known prognostic factors such as tumor size, LN metastasis, and HR status, regardless of histologic type.
The MBC group presented at a younger age than did the IDC group. These results correspond with earlier studies [9-11]. Vu-Nishino et al. [10] demonstrated that women with breast cancer with medullary histology presented at a younger age (mean, 47.5 years vs. 55.6 years), and a significantly higher proportion of patients were classified as very young age (≤35 years). Anderson et al. [18] explained this result using an age-specific incidence rate curve. MBC rates increased rapidly until age 50 and then plateaued, while IDC rates increased rapidly until age 50 and rose slowly thereafter. In our study, age at onset of MBC was younger, and a higher proportion of patients in the MBC group was younger than 35 years, although this difference was not significant (13.5% vs. 9.2%, p=0.330). The age difference between the two groups was smaller than that reported in the Western literature. This difference may be attributable to the fact that Korean women present with breast cancer at younger ages than Western women. According to the Korean Breast Cancer Society, the peak of breast cancer incidence occurs at 40 to 49 years, and a total of 37.1% of women with newly developed breast cancer in 2010 belonged to this group [19]. Therefore, the age gap between histologic groups was smaller in this study.
In previous studies, the effect of tumor size has been controversial. Flucke et al. [20] found smaller tumor sizes in a MBC group than in an IDC group. In contrast, Vo et al. [11] reported that a MBC group had larger tumors than an IDC group (T2 57.0% vs. 27.0%, p<0.001). In our study, tumor size did not differ significantly between groups.
The proportion of patients with LN metastasis was clearly lower in the MBC group without LVI, and patients who did show LN metastasis had no more than two metastases. This finding is consistent with other reports: Flucke et al. [20] showed that patients with MBC had a higher node negative rate (75.0% vs. 47.9%, p=0.0014) and less frequent LVI (3.4% vs. 14.4%, p=0.025) than those with IDC. This finding might be related to the histologic characteristics of MBC, which include dense lymphocytic infiltration especially with CD3, CD8, TIA-1, and granzyme-B positive lymphocytes, and might also be affected by different immune responses in MBC, such as the absence of IgA antibody; the presence of IgG; infiltration of plasma cells; and expression of tumor-specific antigens such as β-actin, ganglioside D3, and HLA-DR [21,22]. These mechanisms could be involved in control of tumor spread and improvement of the prognosis of MBC.
Many previous studies have suggested that typical MBC is associated with a favorable prognosis [7,10,23,24]. Oh et al. [14] reported a difference in the 10-year OS rate of typical MBC and IDC patients, which were 86.0% and 74.7%, respectively, in Korean women. Some researchers have suggested that the good prognosis of MBC is associated with the downregulation of genes involved in cell growth and proliferation, elevated levels of metastasis-inhibiting factors, and low levels of metastasis-promoting factors [4]. However, not all studies have confirmed this finding or have reported similar survival rates for MBC and IDC, including the studies by Fisher et al. and Thurman et al. [25,26]. These authors did not find significant differences between the DFS and OS of patients with MBC and IDC. We also did not find any differences in death or recurrence based on histological type. In addition, in subgroup analyses by pathologic stage, nodal involvement, HR status, HER2 status, and adjuvant treatment, MBC did not differ from IDC in either DFS or OS, as shown in Figures 1, 2 and Table 2. However, in the subgroups with nodal metastasis, patients with IDC had better survival than did those with MBC. This difference may be attributable to the small number of cases.
Another possible explanation for these results may be the implication of LN metastasis in patients with MBC. The MBC group had better nodal staging results (N1 86.5% vs. 58.4%, p<0.001) and microscopic LVI results than did the IDC group (negative 100.0% vs. 70.2%, p<0.001). Rare LN involvement is not only a typical feature of MBC, but also the most important prognostic factor of invasive carcinoma, including medullary type. The significance of the LN status in MBC has been reported in many previous studies [8,23,27]. Martinez et al. [27] showed that 10-year survival rates in patients with MBC with and without LN metastasis were 67.5% and 81.9%, respectively, and Ridolfi et al. [7] reported that patients with axillary LN metastasis to less than three LNs did not die from the disease. Our results were similar. Only 13.5% of MBC patients showed LN involvement, and these were limited to two LNs. Both DFS and OS in patients with MBC with LN metastasis were poorer than in patients without LN metastasis (p=0.010 and p<0.001, respectively), even in patients with IDC. No prognostic factors other than LN metastasis affected survival in the MBC group (data not shown). We could not clearly determine the role of adjuvant treatment in MBC because of the small number of cases. However, among patients treated with adjuvant chemotherapy, those with MBC had better DFS and OS than did those with IDC, unlike the case in patients without chemotherapy, although the difference was not statistically significant. Whether less adjuvant treatment should be given and the prognostic value of adjuvant therapy in this population is still debatable, but on the basis of our results, we suggest that MBC should be treated as other invasive carcinoma according to the National Comprehensive Cancer Network guidelines. Further studies are needed to clarify the implications of adjuvant chemotherapy.
Our study has some limitations. The sample size was small. The MBC group comprised 52 cases, less than 1% of IDC group. We could not perform multivariate analysis to identify prognostic factors in the MBC group because of the small sample size and rare deaths or recurrences. Some immunohistochemistry data, such as the Ki-67 index, CK 5/6 positivity, and epidermal growth factor receptor status, which are important MBC characteristics and might be related to prognosis, were missing. These missing data increase the difficulty in obtaining results of statistical significance.
In conclusion, MBC is a rare breast cancer subtype associated with unique clinicopathologic features, such as rare LN metastasis, ER and PR negativity, advanced tumor grade, and nuclear pleomorphism. The prognosis of MBC is not significantly different from that of IDC, and histologic type in itself was not an independent prognostic factor for invasive breast carcinoma in multivariate analysis. LN metastasis was rare in patients with MBC; however, in patients with LN metastasis, recurrence and death were significantly more common than in patients without LN metastasis or patients with IDC histology. Therefore, patients with MBC require the same intensive treatment as those with IDC, especially patients with LN metastasis, to improve survival.







 XML Download
XML Download