

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Most studies examining the clinical significance of p53 alterations have demonstrated that accumulation of mutant p53 in breast tumors generally correlates with aggressive clinicopathological factors: estrogen receptor (ER) and progesterone receptor (PR) negativity, high proliferation rate, high histological grade, aneuploidy, and poor survival outcome [1-5]. Despite many previous studies demonstrating a poor outcome in cases of p53 overexpression, some studies have shown no statistically significant association with or only a trend towards a poor outcome [6-9]. Recently, a few studies, based on distinct subgroups determined by ER, PR, and human epidermal growth factor receptor 2 (HER2) status, suggested that p53 overexpression plays different prognostic roles depending on ER/PR and HER2 status. Because of the increased prevalence of p53 overexpression in hormone receptor (HR)-negative breast cancers, p53 has been validated as a prognostic marker in HR-negative breast cancers. In addition, the prognostic power of p53 was partially demonstrated in the triple-negative subtype (ER-/PR-/HER2-), which has an aggressive clinical course and a lack of molecular markers [10-12]. Meanwhile, attempts to more accurately predict survival outcomes in ER-positive breast cancers have also been made [13,14]. Therefore, these contradictory results need to be addressed by focusing separately on the prognostic and predictive effects of p53 for each distinct subtype.
A previous study of node-negative breast cancer patients who were not treated with adjuvant systemic therapy demonstrated that there is a correlation between p53 and HER2 overexpression, and their independent poor prognostic effects on long-term survival is commonly due to increased cell proliferation [15]. In terms of an interaction between p53 overexpression and the proliferation rate, a study on p53 accumulation as a variable for prognosis demonstrated that the p53 hazard ratio for distant metastasis paradoxically decreased for higher cell proliferation indexes. This result suggested that p53 accumulation provided prognostic information for a subset of patients with slowly proliferating tumors but not for those with rapidly proliferating tumors [1]. Concomitantly, p53 overexpression has been reported to predict a reduced response to adjuvant treatment [16,17]. However, a retrospective analysis of a series of 1,716 breast cancer patients from the Danish Breast Cancer Cooperative Group 77c study, failed to demonstrate a distinct association between p53 positivity and tamoxifen treatment [18]. Because of the small number of patients in almost all previous studies, investigation of the prognostic and predictive relevance of p53 accumulation with respect to breast cancer subtypes has been inconclusive.
In the present study, we evaluated the prognostic value of p53 overexpression using a nationwide dataset registered by the Korean Breast Cancer Society (KBCS). In subgroup analysis, we also sought to determine whether the prognostic implications of p53 overexpression differ according to the breast cancer subtype and whether the prognostic power of p53 overexpression results from differences in the adjuvant treatment response, as indicated by previous data [16,17].
METHODS
The KBCS has collected breast cancer data since 1996, as described in previous reports [19-21]. Briefly, the Korean Breast Cancer Registry System (KBCRS) is a web-based database prospectively maintained by the KBCS. Breast surgeons in 102 teaching hospitals throughout Korea participate in this program. Essential information includes sex; age; surgical methods; cancer stage based on the American Joint Committee on Cancer classification; immunohistochemical (IHC) staining results for ER, PR, HER2, and p53; adjuvant treatment modalities; and patient survival data. The KBCRS data do not include the type or date of tumor recurrence, only the cause or date of death.
For this study, retrospective IHC data on p53, ER, PR, and HER2 status from 60 hospitals were retrieved from the KBCRS. A total of 15,598 patients diagnosed between 1999 and 2006 were enrolled in this study. Patients who received preoperative systemic therapy or had metastatic breast cancer were excluded. Individual institutions assessed the levels of ER, PR, HER2, and mutant p53 according to their own IHC assay methods. The cutoff value for p53 expression was 10% at all involved institutions, and IHC results for p53 were dichotomized as negative or positive. HR status was determined as positive in cases of ER positivity and/or PR positivity and as negative in cases of both ER and PR negativity. Therefore, all invasive breast cancers were stratified into four subgroups on the basis of IHC HR and HER2 status.
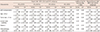
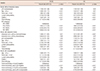
The chi-square test was used to identify differences in variables between groups according to p53 status (Table 1). The prognostic role of p53 for overall survival (OS) and breast cancer-specific survival (BCSS) was estimated by univariate analysis using the Kaplan-Meier method and log-rank test. Multivariate analyses of the prognostic role of p53 in each subtype were assessed using a stratified Cox proportional hazard regression model, and a likelihood test for homogeneity was performed to determine whether the overall hazard ratio should be summarized across all subtypes. In analyses of treatment benefits, first-order interaction terms between p53 overexpression and adjuvant treatments such as hormonal therapy and chemotherapy were entered into a Cox proportional hazard regression model to evaluate their prognostic effect on OS and BCSS. The threshold of statistical significance was 0.05. All statistical analyses were performed using SPSS version 12.0 (SPSS Inc., Chicago, USA) and SAS version 9.2 (SAS Inc., Cary, USA).
RESULTS
p53 overexpression was statistically associated with advanced pathological stage, high tumor grade, ER negativity, PR negativity, and HER2 positivity (Table 1).
The median follow-up duration was 53 months (range, 0-125 months). The 5-year OS rate was 88.0% for p53-positive patients and 91.3% for p53-negative patients (p<0.01). The 5-year BCSS rate was 88.5% for p53-positive patients and 91.8% for p53-negative patients (p<0.01) (Figure 1A). Figure 1 shows the results of subgroup analyses. p53 accumulation was of prognostic value in terms of OS and BCSS, irrespective of tumor size, nodal status, and age. Relatively weak statistical significance for p53 status as a prognostic factor was observed for the group with negative nodal status (p=0.02 and p=0.05 for BCSS and OS, respectively), compared to the group with positive nodal status (p<0.01 for BCSS and OS). With regard to tumor grade, the prognostic significance of p53 accumulation disappeared in the grade 3 group (p=0.21 and p=0.25 for BCSS and OS, respectively). The significant prognostic role of p53 in the HR+/HER2- (p<0.01 for BCSS and OS) and the HR+/HER2+ (p=0.02 for BCSS and OS) IHC subgroups completely disappeared when the HR-/HER2- (p=0.98 and p=0.81 for BCSS and OS, respectively) and HR-/HER2+ (p=0.17 and p=0.10 for BCSS and OS, respectively) IHC subgroups were examined.
Six factors, including tumor size, nodal status, tumor grade, age <35 years, chemotherapy received, and p53 overexpression, were entered into a stratified Cox regression model to evaluate their prognostic effects on survival. The adjusted hazard ratios for all of these factors were significant. The hazard ratio for p53 overexpression was statistically significant only for patients with HR+/HER2- tumors; the hazard ratio of death was significantly higher for patients with p53-positive tumors than for those with p53-negative tumors (OS: hazard ratio, 1.44; 95% confidence interval [CI], 1.08-1.93 and BCSS: hazard ratio, 1.47; 95% CI, 1.09-1.99). Such a difference was not observed in patients with HR-/HER2+ or HR-/HER2- tumors. The hazard ratios of p53 overexpression for OS and BCSS for the HR-/HER2+ and HR-/HER2- subgroups were 1.25 (95% CI, 0.96-1.60) and 1.21 (95% CI, 0.94-1.57), and 0.94 (95% CI, 0.73-1.20) and 0.92 (95% CI, 0.71-1.18), respectively. For the HR+/HER2+ subgroup, the association of p53 overexpression with poor prognosis had borderline significance (OS: hazard ratio, 1.27; 95% CI, 0.98-1.66 and BCSS: hazard ratio, 1.26; 95% CI, 0.96-1.65). By adjustment in a stratified Cox regression model, p53 overexpression was found to be an independent predictor for 5-year OS and BCSS along with conventional prognostic factors such as tumor size, nodal status, tumor grade, age <35 years, and chemotherapy received (Table 2).
Possible interactions between p53 and adjuvant treatment were explored. A significant interaction was observed between p53 expression and hormonal therapy (p=0.002 and p=0.007 for OS and BCSS, respectively) (Table 3), suggesting that the effects of hormonal therapy may differ according to p53 status. Such an interaction was not observed for chemotherapy (p=0.233 and p=0.300 for OS and BCSS, respectively) (Table 3). Although IHC subgroup, p53 overexpression, tumor size, nodal status, tumor grade, age <35 years, and chemotherapy received were significant independent factors affecting OS and BCSS in a model without interaction terms, p53 overexpression alone was not significant in a second model with interaction terms (p=0.268 and p=0.296 for OS and BCSS, respectively) (Table 3). The response to hormonal therapy was greater in p53-negative patients (hazard ratio, 0.49 for OS and BCSS; p<0.01) than in p53-positive patients (hazard ratio, 0.76 and 0.73 for OS and BCSS, respectively; p<0.01), indicating an effect modification of hormonal therapy according to p53 status. Data for 10,073 patients were analyzed in the second model because of missing information on adjuvant treatments.
DISCUSSION
The present study confirmed that nuclear accumulation of the mutant p53 protein correlates with a poor prognosis, as previously observed in several studies. Patients with p53 overexpression had a worse OS than those without p53 accumulation regardless of tumor size, nodal metastasis, and age at diagnosis. The most noteworthy finding in this study was that the prognostic power of p53 varied according to IHC subtypes representing tumor biology: these variations were likely caused by the effect modification of hormonal treatment by p53 status.
Our study demonstrated that the differences in OS and BCSS between patients with and without p53 accumulation reached significance in the HR+/HER2- subgroup, whereas these differences were of borderline significance in the HR+/HER2+ subgroup and of no significance in the HR-/HER2+ and HR-/HER2- subgroups (Table 2). In addition, Kaplan-Meier analysis revealed that p53 accumulation was a significant prognostic factor only for patients with grade 1 and 2 histology, compared with patients with grade 3 histology. Silvestrini et al. [22] suggested that p53 accumulation had no prognostic value for contralateral breast failure or locoregional relapse after radical or conservative surgery plus radiotherapy. However, it was a significant predictor for distant metastasis, which resembled the predictive pattern observed for hormone receptors [1,22]. This result indicates the possibility of interactions between p53 accumulation and hormone receptor status. Therefore, in our study, patients were stratified according to IHC subtypes to evaluate any correlation with survival outcome. The results supported the prognostic value of p53 only for patients with HR+/HER2- tumors. The nonsignificant prognostic value of p53 overexpression for aggressive subgroups such as the HR-/HER2+, HR-/HER2-, and high-grade subgroups can be explained as follows: p53 overexpression is consistently correlated with high malignant potential, but prognostic value may be weakened by the much more prominent effects of strong prognosticators in aggressive breast cancer subtypes. Silvestrini et al. [1] examined a relatively large series of 1,400 patients to validate p53 accumulation as a continuous variable associated with prognosis and showed that the hazard ratio for distant metastasis increased with increasing p53 accumulation up to a value of 12% positive cells and paradoxically decreased thereafter, possibly because of the significant interaction between p53 expression and the cell proliferation index. p53 accumulation is reported to provide prognostic information in a subset of patients with slowly proliferating tumors but not in those with rapidly proliferating tumors [1]. This finding led us to consider the possibility of strengthening the prognostic power of p53 by evaluating p53 in conjunction with ER, PR, and HER2 to elucidate a subtype for which p53 has strong prognostic power. This subgroup was demonstrated to be HR+/HER2- breast cancer in this study.
Experimental approaches to determine a plausible mechanism for the interaction of ER and p53 have suggested the possibility of cross talk between pathways mediated by ER and p53. When deregulated, ERα becomes abnormally proliferative and greatly contributes to the onset and progression of breast cancer [23]. Similar to ERα, the tumor suppressor p53 plays a central role in many cellular processes, such as cell cycle regulation, apoptosis, senescence, and differentiation [24]. Both ERα and p53 play a pivotal role in normal mammary development and in breast cancer oncogenesis. Sayeed et al. [25] proposed a novel mechanism by which ERα opposes p53-mediated apoptosis in breast cancer cells that involves direct binding of ERα to the promoters of p53 target genes, such as survivin and multidrug resistance gene 1. They also showed, in a small-sized retrospective study that analyzed the response to tamoxifen therapy in a subset of 35 patients with ER-positive breast cancer expressing either wild-type or mutant p53, that the presence of wild-type p53 is an important determinant of a positive therapeutic response [26]. Further investigation of the predictive value of p53 for adjuvant endocrine therapy in this study (Table 3) showed a significant association, and the treatment benefit in patients without mutant p53 overexpression was much greater than that in patients with mutant p53 overexpression. The results of our large-scale analysis support the finding by Konduri et al. [26] that the presence of wild-type p53 is an important determinant of a positive therapeutic response in ER-positive breast cancers.
The findings of this study can be applied to several clinical circumstances. First, our findings refine previous luminal IHC biomarker signatures. Millar et al. [13] suggested that predicting the outcome of ER-positive breast cancer is improved using a marker panel comprised of HER2, Ki-67, and p53. They modified the conventional working definition for classifying ER-positive breast cancers, previously based on HER2 overexpression alone, into two distinct subtypes, by analyzing HER2, Ki-67, and/or p53, the five IHC biomarker classifier [13]. In addition, the 2011 St. Gallen International Conference Expert Panel strongly supported the addition of Ki-67 to ER, PR, and HER2, the four IHC biomarker classifier for defining luminal A or B subtypes with a cutoff point of 14% for the Ki-67 labeling index [27]. The present study suggests that p53 overexpression can be incorporated into a more refined luminal IHC biomarker signature and supports the validity of Millar's five IHC biomarker classifier [13]. Second, mutant p53 protein status can be included in the process of determining whether to extend letrozole treatment after 5 years of tamoxifen treatment. This is particularly relevant for patients with HR-positive breast cancer as most instances of relapse and breast cancer mortality occur after 5 years [28]. Although an effective benefit with extended adjuvant letrozole treatment was confirmed irrespective of patient age and nodal status in terms of disease-free survival (DFS) and distant DFS [29,30], the OS advantage was demonstrated only in node-positive breast cancer, casting doubt on the safety of extended adjuvant letrozole therapy. Therefore, when deciding whether to use extended adjuvant letrozole therapy, clinicians and patients should consider the benefit of adjuvant endocrine treatment in addition to the residual risk of relapse, comorbidities, and individual preferences.
One major limitation of this study is that, despite the general consensus on IHC assay methods and the cutoff criteria for receptor positivity in the KBCRS, the IHC results have not been centrally validated. However, it may be justifiable to interpret the clinical role of mutant p53 accumulation as the analyses in this study were performed after dichotomization according to a cutoff value of 10%. An additional limitation of this study is the lack of consideration for the effect of Ki-67 on survival outcomes. The results of this study, therefore, should be interpreted with caution because it is possible that the unique prognostic value of p53 could be confounded by the Ki-67 index given the importance of the proliferation index in HR-positive breast cancer. Finally, an inherent limitation of this study is that data on adjuvant therapy are not mandatory in KBCRS. As mentioned in the methods section, we could only analyze data for 10,073 out of 15,598 patients in the second model with interaction terms. However, importantly, the results of this large, multi-institution analysis further suggests that HR-positive breast cancer patients with IHC p53 accumulation have worse OS and BCSS than those without p53 accumulation. Furthermore, clinicians should note that this finding could result from the association between p53 overexpression and hormonal therapy response and may help when making clinical decisions based on the possible effect modification by p53 status, particularly in patients with HR-positive breast cancer.


 XML Download
XML Download