

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the leading cancer in Asian females [1], and the incidence of breast cancer has been increasing in Asia [2,3]. Approximately 10% of breast cancer cases are thought to be hereditary, and about 25% of these are caused by inherited mutations in the tumor-suppressor genes BRCA1 and BRCA2 (BRCA1/2) [4]. Although less than 5% of all breast cancer patients have mutations in the BRCA1/2 genes, individuals carrying mutations in either one of these genes have a 47% to 55% probability of developing breast cancer and a 17% to 39% risk of ovarian cancer by the age 70 years [5,6]. Given such high risks of cancer in women with BRCA1/2 mutations, alterations in these genes are regarded as some of the most significant predictors for breast cancer development. These mutations are more prevalent among women who have a family history of breast or ovarian cancers, a personal history of breast cancer at young age, or triple-negative breast cancer (i.e., estrogen receptor, progesterone receptor, and HER2-negative) [7-10]. Moreover, the frequency of these genetic mutations varies among ethnic groups and countries [11,12].
Since the identification of the BRCA1/2 genes, a number of studies to evaluate epidemiologic characteristics of BRCA1/2 mutations among diverse ethnicities have been conducted [12-15]. Earlier studies of BRCA1/2 mutations were largely based on Caucasian populations; however, a number of recent studies have focused on Asian patients in order to define the distributions of these genetic mutations in the Asian population [16-29]. Because Asian patients develop breast cancer at a younger age than their Caucasian counterparts [2,30], the contributions of BRCA1/2 mutations in Asians are expected to be different from those in Caucasians.
Knowledge of mutation frequency in the Asian population is vital to optimize the counseling of Asian breast cancer patients and establishing criteria for BRCA1/2 testing. We reviewed the literature regarding BRCA1/2 mutations in Asian breast cancer patients to identify the epidemiologic characteristics of BRCA1/2 mutations in Asian populations.
PREVALENCE OF BRCA1/2 DELETERIOUS MUTATIONS IN ASIAN PATIENTS
Korea
Since the first report of BRCA1 mutations in Korean hereditary breast cancer patients in 1995, there have been approximately a dozen studies evaluating the prevalence of BRCA1/2 mutations in Korea. Until the late 2000s, most BRCA1/2 mutation data were derived from studies involving different genotyping methods at various single institutions. Moreover, the inclusion criteria for genetic testing of breast cancer patients have not been well defined. Therefore, in 2007, the Korean Hereditary Breast Cancer (KOHBRA) study was initiated in order to establish BRCA1/2 carrier cohorts of Korean ethnicity [31].
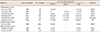
In the KOHBRA study, genotyping of the BRCA1/2 genes was offered to patients with a family history of breast or ovarian cancers. Mutation analysis was also offered to patients with high risk factors for hereditary breast cancer, such as early-onset breast cancer, bilateral breast cancer, a personal history of breast or ovarian cancer, male breast cancer, or cancers involving multiple organs. In the KOHBRA study, the frequencies of BRCA1/2 mutations in nonfamilial high-risk breast cancer patients and familial breast cancer patients were found to be 17.8% and 21.7%, respectively. In another analysis conducted on pooled Korean mutational data of BRCA1/2 genes not covered by the KOHBRA study, 14.9% of high-risk breast cancer patients were found to have BRCA1/2 mutations, and 3.0% of sporadic breast cancer patients had alterations in BRCA1/2 genes [16]. The prevalence of BRCA1/2 mutations in Korean patients is summarized in Table 1.
China
Epidemiologic studies of BRCA1/2 mutations in Chinese breast cancer patients have been performed in mainland China, Hong Kong, Taiwan, and Singapore. Two studies from Singapore predominately included ethnic Chinese patients. Therefore, for this review, the data from these studies will be considered representative of those from an ethnic Chinese population. Mutational analysis was performed in each study using various detection techniques, including single-strand conformation polymorphism (SSCP), protein truncation test, denaturing high-performance liquid chromatography, high-resolution DNA melting analysis, and direct sequencing. The two studies examined large genomic rearrangements (LGRs) of BRCA1/2 genes using multiplex ligation-dependent probe amplification. The Chinese studies initially included a small number of patients at single institutions, but coverage was later expanded to include a larger number of patients across multiple institutions.
Table 2 shows the frequencies of BRCA1/2 mutations in Chinese breast cancer patients. Definitions of familial breast cancer, early-onset breast cancer, or high-risk breast cancer varied among the studies. The prevalence of BRCA1/2 mutations in familial breast cancer and early-onset breast cancer patients ranged from 8.0% to 13.5% and from 8.7% to 11.4%, respectively. In a report by Kwong et al. [32], 7.8% of high-risk breast and/or ovarian cancer patients had BRCA1/2 gene mutations. The report included those with familial breast and/or ovarian cancers, early-onset breast cancer, bilateral breast cancer, triple-negative breast cancer, or multiple cancers. In addition, Suter et al. [33] found that 1.8% of patients with sporadic breast cancer had BRCA1/2 mutations.
Japan
There have been few studies of the prevalence of BRCA1/2 mutations in Japanese breast cancer patients. Mutational analysis was performed by SSCP in the majority of the studies shown in Table 3. In the early 1990s, genotyping was performed for the BRCA1 gene only. The studies showed that 3.5% to 10.0% of familial or high-risk breast cancer patients had mutations in the BRCA1 gene, whereas 0.8% of sporadic breast cancer patients had BRCA1 gene mutations. In reports evaluating BRCA1 in combination with BRCA2 gene mutations, 15.0% to 31.8% of Japanese familial breast cancer patients were reported to have mutations in the BRCA1/2 genes. In all Japanese studies, the mutation prevalence of the BRCA2 gene was higher than that of the BRCA1 gene [21,34-36].
India, Pakistan, Malaysia, Indonesia, the Philippines, and Vietnam
The populations of India, Pakistan, Malaysia, and Indonesia consist of multiethnic groups. Since it is difficult to estimate the prevalence of BRCA1/2 mutations according to ethnic group within these countries, the mutation rates were instead evaluated according to region. The mutational frequencies in India, Pakistan, Malaysia, Indonesia, the Philippines, and Vietnam are shown in Table 4.
In India, there are several reports of small numbers of familial breast cancer patients with BRCA1/2 mutations. The frequency of BRCA1/2 genetic mutations was reported to range from 2.9% to 28.0% among Indian familial breast cancer patients. Furthermore, 2.8% of early-onset breast cancer patients in the Indian population were found to have BRCA1/2 mutations. Notably, the occurrence rates of BRCA2 mutations were lower than those of BRCA1 in almost all Indian studies [22,23,37,38].
The frequency of BRCA1/2 gene was investigated in three breast cancer studies of Pakistani patients [25,39,40]. Rashid et al. [25] reported that 17.0% of familial breast cancer patients have BRCA1/2 gene mutations, whereas Liede et al. [39] found the prevalence of BRCA1/2 mutations to be 6.7% in breast cancer patients in Pakistan. Moreover, 0.67% of Pakistani sporadic breast cancer patients had BRCA1 mutations. The occurrence of these genetic mutations varied across ethnicities within the Pakistani population [24].
In Malaysia, 13.5% of familial breast cancer patients had mutations in the BRCA1/2 genes [41]. In addition, two Malaysian studies reported that 8.1% to 17.0% of patients with early-onset breast cancers had BRCA1/2 mutations. Early-onset cancer was defined as the occurrence breast cancer at the age of ≤35 years in one study [27] and at the age of ≤40 years in another [26].
A study by Purnomosari et al. [28] in Indonesia found that 7.8% of patients at high risk for hereditary breast cancer, such as patients having early-onset breast cancer, familial breast cancers, or bilateral breast cancers, had BRCA1/2 genetic alterations.
LARGE GENOMIC REARRANGEMENT IN BRCA1/2 IN ASIAN BREAST CANCER PATIENTS
Disease-causing mutations in BRCA1/2 genes mainly consist of single base changes, deletions or insertions of a small numbers of bases, or point mutations that result in protein truncation. These mutations lead to significant dysfunction of the BRCA proteins. In addition to alterations in genetic sequence, large rearrangements of DNA segments in the BRCA1/2 genes also contribute to pathogenic mutations. LGRs in BRCA1/2 genes have been studied in various population groups, mainly involving patients in Europe or the United States [43]. Nonetheless, there have been some studies on the contribution of LGR in Asian high-risk breast cancer patients.
In a study of the Singaporean population, 3% (3/100) of high-risk breast or ovarian patients who tested negative for BRCA1/2 deleterious mutations were found to have LGRs in the BRCA genes [44]. On the other hand, a Korean study found that only 0.8% (1/122) of BRCA deleterious mutations-negative high-risk breast cancer patients had LGR in the BRCA genes in the Korean population [45]. Two Malaysian studies found LGRs in the BRCA genes in 2% (2/100) and 0.9% (3/324) of high-risk breast cancer patients, respectively [46,47]. Furthermore, LGRs account for 6.3% of the total mutations in BRCA1/2 genes in a Malaysian cohort [47]. A recent report from southern China found that 0.7% (4/555) of high-risk breast or ovarian cancer patients had LGRs in their BRCA genes, representing 5.8% of overall BRCA1/2 mutations in their cohort [48]. These studies suggest that LGRs in the BRCA genes of Asian high-risk patients amount to less than 7% of all BRCA mutations.
EPIDEMIOLOGIC CHARACTERISTICS OF BCRA MUTATIONS IN ASIAN PATIENTS
The prevalence of BRCA1/2 mutation in Asian patients with familial breast cancer and early-onset breast cancer has been reported to be 8.0% to 31.8%, and 2.8% to 21.4%, respectively (Tables 1-4). The likelihood of mutations in familial breast cancer among Asians was comparable to that of African American or Hispanic Americans although it is lower than that of Ashkenazi-Jews, or Caucasian in North America. The frequency of BRCA1/2 mutations in Asian patients with early-onset breast cancer is similar in range to that in Caucasians or African Americans (Table 5). Direct comparison of BRCA mutation frequency in Asian patients to that of other races cannot be performed due to the differences in the inclusion criteria and variable genotyping methods. Unlike most United States and European studies, only a small number of studies in Asia have been based on complete sequencing of BRCA1/2 genes. The prevalence of BRCA1/2 mutations in Asians is likely to have been underestimated because some genotyping methods adopted in Asian countries are less sensitive than complete DNA sequencing in the detection of BRCA gene mutations [49]. Nonetheless, a United States study concluded that the prevalence of BRCA mutations was similar across diverse ethnicities after complete sequencing of BRCA genes among female patients of various ethnicities who were tested at Myriad Genetic Laboratories, Inc. (Myriad; Salt Lake City, USA) [15]. The study analyzed 1,183 Asian females, which accounted for 2.6% of the study population. Among the Asian patients, 12.7% had BRCA1/2 mutation. The mutation frequencies of BRCA1/2 genes in Western European, Latin American, African, and Middle Eastern females were 12.1%, 14.8%, 15.6%, and 9.4%, respectively. Haffty et al. [50] compared the prevalence of BRCA1/2 mutations in Caucasian, African-American and Korean patients with early-onset breast cancer and found similar BRCA1/2 mutation frequencies of 17% in Caucasian, 14% in African-American, and 14% in Koreans. These studies indicate that mutations of BRCA genes in Asian breast cancer patients are occur at similar rates compared to other racial groups. Except for Pakistani and Indian patients, BRCA2 mutations in the Asian population were detected equally, or more frequently than BRCA1 mutations when compared to other ethnicities. It is a distinct feature of BRCA mutations in Asians because other ethnicities have more BRCA1 mutations than BRCA2 mutations [51].
Notably, the contribution of LGRs to overall BRCA mutations in the Asian population is lower than that reported for other ethnicities. According to an analysis of the Myriad database, which includes 48,456 breast cancer patients of various ethnicities, LGRs in BRCA genes were detected in 1.3% of Asian high-risk patients, comprising 5.3% of all BRCA mutations in their Asian cohorts. The proportion of LGRs in the overall BRCA mutations in the Asian population is lower than in European (9.6%) and Latin American (21.4%) populations [52].
BRCA MUTATION PREDICTION MODELS FOR ASIAN BREAST CANCER PATIENTS
To optimize genetic counseling and provide patient guidelines for BRCA1/2 genotyping, a high-risk group needs to be identified. Several computational models, such as BRCAPRO [53], Couch [54], Myriad II [55], BOADICEA [56], and Manchester [57], have been formulated to determine the probability of a person inheriting mutations in the BRCA genes based on the individual's personal and family history of breast and ovarian cancer. Because these predictive models were constructed using mutation data from Caucasian populations, there have been questions about the accuracy of predicting mutations in other ethnicities variation in the accuracy of such predictive models have also been found between African American and Hispanic populations in the United States [58,59].
Several studies have found a tendency of BRCA1/2 mutation prediction models to underestimate the risk of BRCA1/2 mutations in Asian populations [32,41,60-62]. In a study of Asian Americans, the BRCAPRO and Myriad II models underestimated the proportion of Asian BRCA1/2 mutation carriers by two-fold. Moreover, the underestimation by BCRAPRO was more substantial for BRCA2 than BRCA1 [60]. Both BRCAPRO and Myriad II also underestimated the risk of BRCA1/2 mutations in the Korean population [62]. Additionally, a study from Hong Kong found that BRCAPRO overestimated the number of BRCA1/2 mutation carriers in females with a carrier probability of ≥20%, but underestimated it in women with a carrier probability of <20%. Both Myriad II and BOADICEA underestimated the proportion of BRCA1/2 mutation carriers in Chinese women. Based on these studies, the existing BRCA mutation prediction models are considered inappropriate as guidelines for testing for BRCA gene mutations in Asian individuals because these models underestimate the likelihood of BRCA1/2 mutations in Asian populations.
FUTURE DIRECTIONS
Genetic testing for BRCA1/2 mutations has become an integral part of patients care. Substantial research has been conducted on BRCA1/2 genetic mutations in Asian countries to gain information on the diversity of these genetic mutations across different ethnicities. Until recently, BRCA1/2 mutational analyses in Asian regions have been conducted in single institutions with different patient selection criteria and genotyping methods. Therefore, mutation frequencies have been inconsistent among studies even when they were performed in the same country. This has led to difficulties in genetic counseling in Asian breast cancer patients. The Hong Kong Hereditary and High Risk Breast Cancer Program (HRBCP), and the KOHBRA are national studies designed to provide accurate data on BRCA1/2 gene mutations for Asian populations. In addition to these efforts, Korea, Japan, China, Hong Kong, Indonesia, Malaysia, and Singapore have launched the Asian BRCA Consortium (ABRCA) to study hereditary breast and ovarian cancer. A more comprehensive understanding of BRCA1/2 mutations in the Asian population will be established through these international collaborations.
CONCLUSIONS
The prevalence of BRCA mutations in Asian breast cancer patients is similar in range to that of other ethnic populations. BRCA2 mutations were detected equally, or more frequently than BRCA1 mutations in Asian populations with the exception of Pakistan or Indian breast cancer patients. The contribution of LGRs to overall BRCA mutations in the Asian population is lower than that reported for other ethnicities. Existing statistical models for predicting BRCA1/2 mutations may not be applicable to Asian population as they tend to underestimate the risk of these genetic mutations, particularly for predicting BRCA2 gene mutations.




 XML Download
XML Download