

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is a leading cause of cancer-related death in woman worldwide. Mammography and other diagnostic tools permit earlier detection, while adjuvant chemotherapies extend survival. Death from breast cancer occurs primarily through distant metastasis. Nearly 30% of patients with axillary node-negative breast cancer and almost 50% of those with axillary node-positive breast cancer will eventually experience tumor recurrence following surgical resection with adjuvant chemotherapy due to occult micrometastatic cells in their blood [1]. Metastasis stems from minimal residual disease (MRD) and the presence of single disseminated or circulating tumor cells (CTC) that are undetectable even by high resolution imaging technologies [2,3].
Disseminated tumor cells (DTC) are known to predict unfavorable outcomes in breast cancer patients, but the detection of DTC in the bone marrow is cumbersome, painful and invasive [4,5]. Many clinicians are turning to CTC research because CTC detection is well tolerated, minimally invasive and easily reproduced. The value of peripheral blood CTC in prognosis was first evaluated in patients with metastatic breast cancer and more recently evaluated in the general breast cancer population [6-10].
Cytokeratin-20 (CK-20) presents a valid marker for CTC in peripheral blood because it is not expressed in normal healthy hematologic tissues or in benign breast disease, including inflammatory breast disease therefore, CK-20 is used as a marker of hematogenous micrometastasis and a reverse transcriptase polymerase chain reaction (RT-PCR) target for the detection of breast CTC in patients with breast cancer [11-13].
Breast cancer can be classified in intrinsic subtypes according to distinct gene profile [14,15]. This molecular classification includes four main subtypes of breast cancer: luminal A subtype, luminal B subtype, human epidermal growth factor receptor 2 (HER2) subtype, and basal-like tumors [16]. Breast cancers have different clinical features according to their intrinsic subtypes, accordingly, they may have a different prognostic CTC value according to own subtype [17]. CTC can exhibit different characteristics compared to primary tumors [18]. Until now, few studies have addressed the prognostic significance of CTC according to breast cancer molecular subtype, particularly with regard to long-term follow-up.
In this study, we analyzed the relationships between CK-20 mRNA-positive CTC in the peripheral blood and previously recognized factors in operable breast cancer, and we evaluated the different prognostic significance of CK-20 mRNA-positive CTC according to the 4 breast cancer molecular subtypes.
METHODS
Materials
Peripheral blood samples were obtained from breast cancer patients who underwent surgery at Korea University Anam Hospital from April 1997 to May 2003. Each patient provided informed consent prior to the blood collection. The samples were collected as described to study the sensitivity of CK-20 mRNA expression for detecting CTC and the relationship between the established prognostic parameters and CK-20 mRNA-positive CTC in breast cancer [12,19]. Based on retrospective reviews of medical records, patients were selected for this study according to the following inclusion criteria: 1) female gender; 2) diagnosis of invasive ductal carcinoma; 3) stage I-IIIA according to the American Joint Committee on Cancer staging system (6th edition) defined as an operable breast cancer; 4) data available to determine estrogen receptor (ER), progesterone receptor (PR), and HER2 status; and 5) no previous surgery or other treatments for the primary tumor. Accordingly, 166 patients met the criteria and were entered into this study.
All patients included in this study received treatments judged appropriate for the stage and hormone receptor status of their tumors. Surgical procedures included breast-conserving surgery and modified radical mastectomy. Breast-conserving surgery included lumpectomy, quadrantectomy and wedge resection with axillary lymph node dissection. All patients who underwent breast-conserving surgery received radiation therapy and all ER+ patients received tamoxifen therapy (20 mg daily for 5 years). Patients with HER2-positive tumor did not receive adjuvant treatment with trastuzumab (Herceptin®; Genentech, San Francisco, USA).
Sample collection and RT-PCR amplification of CK-20 mRNA
The blood samples (10 mL) were collected just prior to surgery under general anesthesia from the ante-cubital vein after several milliliters of blood were drained to avoid contamination with skin epithelial cells. The blood samples were collected in ethylenediaminetetraacetic acid-treated tubes, placed on ice, and transported immediately to the laboratory for RNA isolation. RT-PCR amplification of CK-20 mRNA was performed as previously described [12,19].
Immunohistochemistry for ER, PR, HER2, and molecular subtypes
ER (DAKO, Glostrup, Denmark) and PR (DAKO) status were recorded as positive if >1% of the tumor nuclei were immunoreactive. Otherwise, ER and PR were recorded as negative. For HER2 status (Labvision, Fremont, USA), 0 and 1+ were considered negative and 3+ was considered positive by immunohistochemistry (IHC). Fluorescence in situ hybridization (FISH) was not performed for 2+ HER2 status by IHC, and HER2 2+ patients were excluded from the study. Molecular subtypes were assigned according to ER, PR, or HER2 status: luminal A (ER+ and/or PR+, HER2-), luminal B (ER+ and/or PR+, HER2+), triple negative (ER-, PR-, HER2-), and HER2 (ER-, PR-, HER2+).
Statistical analysis
The relationships between CK-20 mRNA-positive CTC and clinical factors were evaluated using Fisher's exact test and Pearson's chi-square test. Metastasis-free survival (MFS) and overall survival (OS) according to molecular subtypes were estimated using the Kaplan-Meier log-rank method. To evaluate independent prognostic factor and relative risk, multivariate analyses were performed using the Cox proportional hazards model and logistic regression. All statistical tests were performed at the 5% significance level (p<0.05). All statistical analyses were performed using SPSS version 18.0 for Windows (SPSS Inc., Chicago, USA).
RESULTS
Patients characteristics
The characteristics of the 166 patients are presented in Table 1. The patients' mean age was 49.5±10.4 years (range, 26-78 years). The median follow-up time was 100.6 months (range, 0.4-163.9 months). The CK-20 mRNA-positive CTC was detected in 37 (22.3%) of 166 patients. According to breast cancer subtype, 73 patients were identified as luminal A (44.0%), 40 as luminal B (24.1%), 36 as triple negative (21.7%), and 17 as HER2 (10.2%).
No significant differences were observed in the distribution of CTC-positive status according to molecular subtype of breast cancer. CTC-positive status was not significantly associated with any previously established prognostic factor and was correlated only with recurrence and breast cancer-specific death in operable breast cancer (p=0.023 and p=0.042, respectively) (Table 1).
Prognostic impact of CK-20 mRNA-positive CTC before surgery
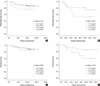
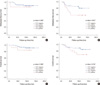
Overall, locoregional recurrences were observed in 9 patients (5.4%), while systemic recurrences were seen in 27 patients (16.3%). During follow-up, 20 breast cancer-specific deaths occurred (12.0%). Patients with positive CTC status had significantly shorter MFS and OS in operable breast cancer (log-rank, p=0.013 and p=0.042, respectively) (Figure 1). Positive CTC was not associated with MFS or OS in patients with either early breast cancer (tumor, node, metastasis [TNM] stage I, II) or advanced breast cancer (TNM stage IIIA) (log-rank, p>0.05) (Figure 2). Positive CTC was not significantly related with MFS or OS in the lymph node-negative patient group, and also was not related with OS in lymph node positive patient group (log-rank, p>0.05) (Figure 3). Positive CTC was associated with shorter MFS in the lymph node-positive patient group only (log-rank, p=0.037) (Figure 3B).
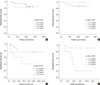
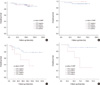
Luminal A and luminal B subtypes did not differ significantly in MFS (log-rank, p=0.443 and p=0.331, respectively) (Figure 4A, B) and OS (log-rank, p=0.848 and p=0.494, respectively) (Figure 5A, B) according to CTC-positive status. Among patients with triple negative breast cancer, those with CTC-positive status had shorter MFS and OS (log-rank, p=0.051 and p=0.042, respectively) (Figure 4C, 5C). Patients with CTC-positive status in the HER2 subtype breast cancer group also had shorter MFS and OS (log-rank, p=0.004 and p=0.026, respectively) (Figure 4D, 5D).
Based on Cox multivariate analysis, CTC status independently predicted MFS (odds ratio [OR], 2.263; 95% confidence interval [CI], 1.006-5.092; p=0.048) (Table 2) but not OS (OR, 2.363; 95% CI, 0.905-6.169; p=0.079) (Table 2). Among the molecular subtypes of operable breast cancer, only the triple negative subtype independently predicted MFS (OR, 2.910; 95% CI, 1.151-7.359; p=0.024) (Table 2) and OS (OR, 5.077; 95% CI, 1.650-15.623; p=0.005) (Table 2).
DISCUSSION
Using univariate analysis, we found no correlation between CK-20 mRNA-positive CTC and any previously established prognostic factor in operable breast cancer (Table 1). Recent reports present HER2 status as the only primary tumor characteristic that reliably predicts the presence of CTCs [9,20]. Tao et al. [9] used a cell enrichment technique with laser scanning cytometry to detect CTC in the peripheral blood. They considered a 2+ staining pattern for HER2/neu as a positive value and did not perform FISH to test the extent of gene amplification. Lang et al. [20] used the CellSearch® system (Veridex, Warren, USA) to detect CTC in 30-mL peripheral blood samples and used FISH to further investigate all cases with 2+ and 3+ staining patterns for HER2 to confirm the presence of gene amplification. However, these results should be interpreted with caution due to the small number of cases with HER2 positive status (n=13) in that study. We declined to determine HER2 gene amplification using FISH and excluded patients with HER2 2+ status from our study. This may explain the difference between our results and theirs. Also, the difference between our result and theirs is well explained by differences in experimental techniques.
We also found that in patients with operable breast cancer, CK-20 mRNA-positive CTC predicted shorter MFS and OS, especially in the triple negative and HER2/neu subtypes. Ignatiadis et al. [17] reported for the first time that the presence of CK-19 mRNA-positive CTC predicted poor clinical outcomes (relapse and death) in patients with ER-negative but not ER-positive early breast cancer. They explained this as a result that in the ER-negative group micrometastatic cells could be targeted only by adjuvant chemotherapy, whereas in the ER-positive subgroup they could be controlled by both adjuvant chemotherapy and hormone treatment. Similarly, we found that our patients with CK-20 mRNA-positive CTC had shorter MFS and OS (log-rank p<0.05; data not shown) in the ER-negative subgroup only. Ignatiadis et al. [17] also suggested that the presence of CK-19 mRNA-positive CTC was associated with shorter DFS and OS in the triple negative and HER2 positive subgroups but not in the ER-positive/HER2 negative subgroup; this finding is in accordance with our findings [17]. There are some possible explanations for this result. Triple negative and HER2 breast cancer subtypes are well known for their poor prognosis and aggressive behavior [14-16]. Brain metastasis is more often observed from these breast cancer subtypes than other subtypes [21,22]. As such, these subtypes might give CTC in the peripheral blood more opportunities to develop local recurrence with eventual dissemination to distant sites due to failure of systemic therapy and the unknown intrinsic propensity to distant metastasis. Because HER2 breast cancer and triple negative breast cancer are subgroups of ER-negative breast cancer, these patients did not receive hormone therapy after their surgical procedures. The discontinuity in systemic treatment after surgery may potentially provide time for the CTC to progress and migrate to distant sites. We did not treat our patients with HER2 positive breast cancer with trastuzumab after surgery because the positive trial results were not yet published at that time [23,24]. This may explain in part why patients in the HER2 breast cancer subgroup with CK-20 mRNA-positive CTC had shorter MFS and OS. Further study is required to determine the prognostic significance of CTC in patients with HER2-positive breast cancer who are treated with trastuzumab.
Our results suggest that the prognostic value of preoperatively detected CTC differs according to the molecular subtype of breast cancer. Interestingly, however, the biological characteristics of the CTC do not necessarily represent the molecular subtype of the primary tumor. In fact, a change in CTC character with respect to the primary tumor, especially HER2, may serve to monitor responses to targeted therapy and chemotherapy and help clinicians select patients who are most likely to benefit from secondary adjuvant treatment [18,25,26]. Pestrin et al. [26] reported that 29% (8/28) of HER2-negative primary tumors had HER2-positive CTC and that 42% (5/12) of HER2-positive primary tumors had HER2-negative CTC. They then suggested that a subset of patients with HER2-negative primary tumors develops HER2-positive CTC during disease progression [26]. Unfortunately, we did not characterize the CTC in this study because the necessary RT-PCR reagents were not available.
Methods to detect CTC in the peripheral blood include RT-PCR using mRNA, CellSearch® (Veridex), CTC-chip, AdnaTest BreastCancer™ (AdnaGen, Langenhagen, Germany), CAM method, MAINTRAC® analysis (SYMPO, Bayreuth, Germany), Membrane microfilter assay, Fiberoptic array scanning technology (FAST), Epithelial immunospot assay (EPISPOT), and others [27,28]. Although RT-PCR has high sensitivity, its specificity is generally low and results in higher false positive rates, and molecular profiling assays of CTC could not be conducted [18,22,24]. However, we used the CK-20 mRNA with RT-PCR method to detect CTC in the blood because our previous reports revealed that CK-20 was not expressed at all in normal healthy individuals or in patients with benign disease. This finding showed that CTC as detected by the CK-20 assay originate uniquely in malignant foci [12,19]. Many efforts have been made to enhance the sensitivity and specificity of RT-PCR for detecting CTC in the peripheral blood [13,18]. Giribaldi et al. [13] developed a real-time RT-PCR method for detecting CK-20 cells with two novel features: 1) a primer overlapping two adjacent exons to inhibit nonspecific amplifications and 2) a non-end-point first-round amplification to increase sensitivity. In addition, the use of multi-marker real-time RT-PCR assays may potentially improve the method even in the case of a single down-regulated gene [18].
This study is limited most significantly by its retrospective design, which reduces the confidence of the study data. In addition, although we intended to assess the prognostic significance of CTC in the peripheral blood according to breast cancer molecular subtype, we did not perform FISH to establish HER2 amplification in patients with HER2 2+ status. Instead, we excluded these patients from this study. Third, our study is limited by its small number of patients. Notwithstanding these limitations, to our knowledge, the current study is the first to evaluate the prognostic value of CK-20 mRNA-positive CTC according to molecular subtype based on long-term follow-up of patients with operable breast cancer. Our results may prompt other researchers to seek further correlations between CTC and breast cancer subtype. In the near future, CTC may become a useful parameter for predicting the prognosis of patients with operable breast cancer, particularly those with the triple negative and HER2 subtypes.
CK-20 mRNA-positive CTC may present a clinically relevant biological marker of tumor progression, especially in the triple negative and HER2 subtypes of operable breast cancer. Large scale prospective trials may be justified to assess the value of CTC determinations in planning treatment for and predicting outcome in these cancers.



 XML Download
XML Download