

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast carcinoma is one of the most common neoplasms in women and is a leading cause of cancer-related deaths worldwide [1]. In Egypt breast cancer is the most common cancer among women, representing 18.9% of total cancer cases (35.1% in women and 2.2% in men) among the Egypt National Cancer Institute (NCI) series of 10,556 patients for 2001 (World Health Organization Regional Office for the Eastern Mediterranean, Cairo, Egypt), with an age-adjusted rate of 49.6 per 100,000 in the population. However, this represents the hospital-based data of referral tertiary centers and does not represent all breast cancer cases in Egypt.
Significant breast cancer risk factors include: age, menarche at an early age, menopause at late age, late age for the first pregnancy, obesity, dense breast tissue, oral contraception use, hormone replacement therapy, alcohol, tobacco smoke, diet, family history, lactation, and prior history of benign breast disease [2]. A number of genes, including BRCA1 and BRCA2, HER2/neu, and p53, have been linked to breast cancer susceptibility and development [3].
Oxidative stress is due to a disturbance in the balance between the production of a reactive oxygen species (ROS) and the efficiency of the antioxidant defense. In other words, oxidative stress results in an excessive production of ROS which overwhelms the antioxidant defense system or when there is a significant decrease or lack of antioxidant defense [4].
Experimental evidence revels that ROS are involved in the initiation and promotion of carcinogenesis, where inactivation or loss of certain tumor suppressor genes have occurred [5]. The levels of free radical molecules are controlled by various cellular defense mechanisms, consisting of enzymatic components (catalase, glutathione peroxidase, superoxide dismutase) and non-enzymatic components (vitamin E, vitamin C, and glutathione components) [6].
Anthracyclines rank among the most effective anticancer drugs ever developed [7]. Most patients with breast cancer are treated with a combination of the anticancer chemotherapy drugs of 5-fluorouracil, doxorubicin, and cyclophosphamide (FAC). These antineoplastic agents cause a reduction in antioxidant levels because their toxicity increases the peroxidation of the unsaturated fatty acids of membrane phospholipids [8]. Their main adverse effects may be heart damage (cardiotoxicity) and vomiting which considerably limits their usefulness. The molecular pathogenesis of anthracycline cardiotoxicity remains highly controversial, although the oxidative stress-based hypothesis involving the intramyocardial production of ROS has gained the widest acceptance [9]. Therefore the current study aimed to investigate the effect and association of breast cancer on oxidative stress, as well as hepatic and cardiac biomarkers in patients receiving combination chemotherapy treatment.
METHODS
Drugs and instruments
Doxorubicin for intravenous administration was obtained from Ebwe Pharma Company (Cairo, Egypt) and cyclophosphamide and 5-flurouracil from EIMC Pharmaceuticals Company (Cairo, Egypt). Chemicals for sensitive biochemical assays were obtained from Randox Laboratories Ltd., Crumlin Company, Antrim United Kingdom, Bio-diagnostic Company (Giza, Egypt) and Spectrum Company for Biotechnology (Cairo, Egypt). Distilled water was used for the biochemical assays. Spectrophotometric measurements were done with T80 UV/Vis spectrophotometer (PG Instruments Ltd., Wibtoft, UK).
Patients and experimental protocol
This study included 40 breast cancer patients from the Department of Oncology of Beni-Suef University Hospital. The inclusion criteria for this study were: the presentation of a palpable mass in the breast that was observed with mammography that was later histologicaly diagnosed. Most of the patients were clinically categorized as stage II and some were in stage I, stage III according to the classification of the Union for International Cancer Control (UICC 1997). The cases were classified according to TNM classification and tumors were histologicaly diagnosed in most cases as invasive ductal and invasive lobular and a few other types are presented in a Table 1 according to Rajneesh et al. [10].
The patients were classified into two groups. The first were recent breast cancer patients that had clinical and histopatological evidence of breast cancer and were receiving neither chemotherapy nor hormonal treatments. The second group was FAC treated breast cancer patients who mostly received 2 FAC cycles (5-flurouracil 500 mg/m2, doxorubicin 50 mg/m2, and cyclophosphamide 500 mg/m2).
Twenty healthy women served as control normal group for the breast cancer group. Cases with illness that are associated with altering free radical levels in healthy and cancer patients (such as diabetes, hypertension, myocardial ischemia, myocardial infarction, renal disorders, pancreatic disorders, pulmonary disease, and pregnancy) and patients with fibroadenoma or with any previous treatment were excluded from this study.
Both the patients and control normal groups had a similar socioeconomic status and dietary pattern. A medical history, physical examination and laboratory tests were obtained from all subjects. None of the subjects included in the study had a history of substance abuse or dependence, serious medical conditions, severe head injury or seizure disorders.
Ethics approval
The materials in our study are human blood sample from normal, breast cancer and treated with FAC, which are giving during breast cancer treatment.
Moreover, our study contains no private information on patients. So, our work has no problems in causing any ethical issue or violation of human rights. Informed consent was obtained from all participants and the protocol used in our study was approved by the Committee of the Beni-Suef University (Beni-Univ-MSc 171-2010).
Serum collection and preparation
Venous blood samples were collected by arm puncture in patients, controls and the FAC treated group 24 hours after the administration of the last dose. Blood (3 mL) was collected, allowed to clot, and centrifuged at 3,000×g for 15 minutes. The separated serum was then stored at -4℃ and the clarified serum preparations were used for biochemical analysis.
Biochemical analysis
Catalase was assayed by the Cohen et al. [11] method based on the reaction of catalase with a known quantity of H2O2. The remaining H2O2 reacts with a dye to form a chromophore with an intensity of color inversely proportional to the amount of catalase in the original sample. The glutathione reduced (GSH) estimated by Beutler et al. [12], this estimation based on the reduction of 5, 5' dithiobis (2-nitrobenzoic acid) (DTNB) with GSH. The reduced chromogen is directly proportional to the GSH concentration and its absorbance can be measured at 405 nm. Nitric oxide (NO) was measured according to Miranda et al. [13], and lipid peroxide (malondialdehyde) was measured according to Satoh [14], by an estimation of thiobarbituric acid reactive product which measured colorimetrically at 534 nm. Analysis of liver enzymes alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were based on the measurement of pyruvate hydrazone and oxaloacetate hydrazone colorimetrically at 546 nm. Serum creatine kinase (CK) was determined using the Burtis and Ashwood [15] method. The catalytic activity was determined from the rate of NADPH formation, measured at 340 nm by means of the hexokinase (HK) and glucose-6-phosphate dehydrogenase (G6PDH) coupled Reactions. Determination of serum lactate dehydrogenase (LDH) via catalyzes the reaction between pyruvate and NADH to produce NAD and L-lactate. It is determined by measuring a decrease in the absorbance of 340 nm. Serum creatinine was assessed by a reaction with picric acid in alkaline solution to form a colored complex. Uric acid was measured according to Fossati et al. [16].
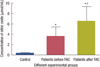
Statistical analysis was carried out using Graph Pad Instat software version 5 (ISS-Rome, Rome, Italy). One-way analysis of variance followed by Tukey-Kramer multiple comparisons post-test were used in an analysis of the data. Values of p<0.05 were regarded as significant. Data were expressed in tables and figures as mean±SEM. The number of patients for each group was 12. Means that shared the same letter were not significantly different. Means that have different letters were significantly different (p<0.05).
RESULTS
Results are summarized in tables and figures as follow: Table 1 shows the classification of breast cancer patients who participated in our study. Data shows that MDA level increased significantly in breast cancer patients compared to normal control. FAC chemotherapy triggered an enhancement in the lipid peroxidation compared to healthy controls (Table 2, Figure 1).
The serum NO increased in breast cancer patients before treatment as compared to normal control. FAC chemotherapy caused an increase in NO compared to patients before treatment and to healthy controls (Table 2, Figure 2).
Serum antioxidants catalase activity and the level of GSH were significantly diminished in breast carcinoma patients before treatment as compared to normal control. These changes more declined with FAC chemotherapy as compared to breast cancer patients and healthy controls (Table 2, Figures 3 and 4).
FAC chemotherapy induced a significant increase in the activities of CK compared to patients before treatment and healthy controls. Moreover the activity of LDH was elevated in FAC treated patients as compared to healthy controls (Table 3, Figures 5, and 6).
The liver enzymes ALT and AST activities and renal creatinine and uric acid levels show no change in patients before treatment or after receiving FAC in comparison to healthy control (Table 4).
DISCUSSION
In our study we investigated the effect of breast cancer on the levels of various enzymes with antioxidant activities and oxidative stress markers NO and lipid peroxidation and the effect of FAC treatment on these parameters.
Several reports have presented evidence that ROS are involved in the etiology and progression of breast cancer [17]. However, most studies are based on breast cancer culture cells or experimental data. Moreover, few studies have investigated the change of oxidative parameters in patients with breast cancer after chemotherapy and the results are also controversial. Therefore, our study provides the most significant data.
ROS plays an important role in tumor initiation, and in a healthy organism ROS levels are controlled by endogenous mechanisms including glutathione and enzymes like catalase. Elevated ROS levels can initiate DNA damage, and might ultimately lead to carcinogenesis [18].
The present results showed an increased NO and lipid peroxidation in breast cancer patients with a decreased antioxidant defense of catalase and GSH. This may be due to increased free radical generation that damage several cellular molecules. These results are in accordance with Prabasheela et al. [19], and Kasapović et al. [20] who found that catalase and superoxide dismutase activity were found to decrease indicating enhanced free radical activity in breast cancer patients while the antioxidant defense mechanism is weakened. Cancer cells generate a ROS, and biochemically have low levels of antioxidant enzyme in most animal and human cancers.
The high levels of NO production in breast cancer and chemotherapy may result in high cytotoxic activity. Consequently the mechanism of inhibiting the production of NO is important for the improvement of breast cancer and chemotherapy. NO promotes cancer progression by activating several oncogenic signaling pathways such as extracellular signal-regulated kinases and phosphoinositide 3-kinases [21].
NOS2 upregulation and elevated NO production affect the redox state of cells and can induce protein, lipid, and DNA modifications. A release of variable amounts of NO into the tumor microenvironment can activate oncogenic pathways, including Akt, epidermal growth factor receptor, and c-Myc signaling pathways, and stimulate tumor microvascularization. More recent findings suggest that NO induces stem cell-like tumor characteristics in breast cancer [22]. The significantly elevated NO in our data was associated with breast cancer as compared with control and that increment was aggravated with chemotherapy.
This work provides novel evidence that NO modulates the progression of breast cancer in association with oxidative stress markers in patients with breast cancer.
Our data elucidates that FAC chemotherapy increases the already existing oxidative stress in breast cancer patients. Alshabanah et al. [23] reported a decrease in the gene expression levels of glutathione peroxidase (GSHPx), catalase, glutathione reductase (GR), and glutathione transferase (GST) in liver tissue with the cumulative dose of doxorubicin with a decrease in their activity in the serum. The data showed that doxorubicin not only increased free radical formation but also decreased its ability to detoxify a ROS. The formation of superoxide radicals together with NO might form peroxynitrite induced by doxorubicin which causes tissue damage leading to an increase in the levels of thiobarbituric acid substance.
These chemotherapeutic drugs are hydrophilic and cannot penetrate the inner membrane of cells where they would be reduced by NADH located on the inner membrane surface [24,25]. Chemotherapeutic drugs, particularly doxorubicin used in FAC treatment are able to enter the outer mitochondrial membrane and enter the cytosol. Intramolecular rearrangements result in the formation of a lipophilic deoxyaglycone that can penetrate the inner membrane of the mitochondria. There doxorubicin competes with coenzyme Q10 as an electron acceptor and diverts electrons to molecular oxygen resulting in the formation of super oxide radicals [25]. Doxorubicin intercalates DNA coils and interferes with normal cellular metabolism through a diverse set of biochemical mechanisms that may explain its toxicity. It causes an increase in the peroxidation of unsaturated fatty acids of membrane phospholipids which lead to a decrease in the level of antioxidants and generate a high level of oxidative stress. In addition, doxorubicin is able to divert electrons from the mitochondrial electron transport system in addition to generating ROS at cellular sites.
Our results indicated that enhanced cardiac enzymes CK and LDH after FAC treatment which evidenced that cardiotoxicity is the main side effect of chemotherapy particularly doxorubicin used in FAC treatment. These results are in agreement with the results by Kaithwas et al. [26]. The increment in serum LDH level suggests an increased leakage of this enzyme from mitochondria as a result of toxicity induced by treatment with doxorubicin [27]. It is recently reported that the doxorubicin-induced free radical generation triggers membrane peroxidation and the disruption of cardiac myocytes, which can led to an increased release of CK in the serum [27].
The heart is more susceptible than other tissues to the oxidative stress produced by ANTs. Several responses have been proposed; ANTs have been shown to be retained within cardiomyocytes more than other cell types. ANTs are thought to enter the mitochondria and to inhibit the respiratory chain by binding to cardiolipin, which is a relatively cardiospecific phospholipid that is rich in polyunsaturated fatty acids and that is found in the inner mitochondrial membrane. Cardiolipin has a high affinity for ANTs [28].
Cardiac tissue has weak antioxidant activity, since it lacks catalase, and some researcher have shown that doxorubicin selectively down-regulates glutathione peroxidase suggesting that cardiomyocytes are exposed to high levels of hydrogen peroxide. In addition, cardiomyocytes are rich in mitochondria, which represent up to 50% of cardiomyocyte mass which serve as both source and target of ROS [29,30]. Moreover, the important role has been attributed to exogenous NADH dehydrogenase.
Unlike cardiac mitochondria, liver mitochondria lack the NADH-related pathway of reducing equivalents from cytosol to the respiratory chain. As a result liver mitochondria do not generate significant amounts of ANT semiquinones [30].
The current study provide novel data about the relation of breast cancer, oxidative stress, cardiac and hepatic function biomarkers with and without the combined formula used in chemotherapy for an Egyptian breast cancer patient.
It could be concluded that breast carcinoma leads to oxidative stress evidenced by an increased NO level and decreased catalase and glutathione which enhance lipid peroxidation level. The treatment by FAC chemotherapy exaggerates oxidative stress leading to cardiotoxicity so monitoring serum oxidative markers and cardiac enzymes is highly recommended.
The data revealed indicated that oxidative stress and cardiotoxicity development may ensure breast cancer progression, possibly mediated through catalase, GSH, MDA, NO, LDH, and CK activity.
Future studies needs to investigate the uses of potent antioxidant compounds to compete the oxidative stress of breast cancer and chemotherapy.







 XML Download
XML Download