

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A family history of cancer is a predisposing factor for other primary cancers. For example, familial breast cancer and hereditary nonpolyposis colorectal cancer are associated with increased risk of pancreatic cancer [1-4]. The positive association between a family history of pancreatic cancer and risk of lymphoma and ovarian cancer is another example [5]. Since BRCA1 and BRCA2 are involved in pathways that regulate DNA repair, cell-cycle progression, and apoptosis, mutations of the genes predispose to breast, ovarian, and other primary cancers such as pancreatic, stomach, biliary tract, and prostate cancer [6-9]. Familial cancers other than breast or ovary are also associated with mutations of BRCA1 or BRCA2 [10-12].
BRCA1 or BRCA2 mutations contribute to the earlier onset of breast cancer [13-15]. A higher prevalence of mutation is also observed in patients with a family history of breast or ovarian cancer, male breast cancer, and bilateral breast cancer [16-18]. A comparative study of population differences in the prevalence of BRCA mutation showed nearly identical frequencies of deleterious mutation across populations, but deleterious mutations were associated with higher risk of secondary malignancies [19].
Taken together, BRCA mutations influence the development of second primary cancers other than breast or ovary cancer. This effect was observed in patients with mutations or in family members of probands. The risk factors mentioned above are related to a higher mutation incidence. In Korea, previous studies have been confined to show the relationships between BRCA mutation and the risk factors. One study showed a higher risk of secondary malignancies among patients with deleterious mutation [19], but the relationship between BRCA mutation and other primary cancers in family members has not been investigated. In this study, we conducted BRCA genetic testing in breast cancer patients with risk factors for carrying mutations. We then analyzed the relationships between mutations and prevalence of other primary cancers in family members including probands.
METHODS
From April 2008 to May 2011, a total of 272 patients were enrolled at a single institute, the Samsung Medical Center. Patients with breast cancer who carried at least one of the following risk factors were included: reported family history of breast or ovarian cancer at any age; 40 years or younger at diagnosis; bilateral breast cancer; or male gender. The members of the family included first- and second-degree relatives, first cousins, and the probands themselves. After informed consent was acquired, genetic counseling was primarily focused on personal and family history of all cancers. The familial pedigree was organized from the information by a research nurse. If any member had a history of cancer other than breast or ovary, the family was regarded as positive for other primary cancer. After excluding 34 patients who refused to participate in the study or provided insufficient information, the number of eligible patients was 238.
BRCA mutation analysis was performed at the Department of Laboratory Medicine and Genetics, Samsung Medical Center. Genomic DNA was extracted and purified from peripheral blood leukocytes. The whole exons and their flanking intrinsic sequences of the BRCA1/2 genes were amplified by polymerase chain reaction. The amplified products were directly sequenced and the sequences were compared with reference sequences using Sequencher software (Gene Codes Co., Ann Arbor, USA). The genetic mutations analyzed were confined to deleterious mutations such as frameshift or nonsense mutation in accordance with the breast cancer information core (BIC) database (http://research.nhgri.nih.gov/bic). And variants of unknown significance were excluded. Genetic testing of high risk breast cancer patients was approved by the Institutional Review Board of Samsung Medical Center (2010-09-006-001).
Fisher's exact or chi-square tests were used to analyze the relationships between the distributions of risk factors and BRCA mutation. These tests were also used to assess the relationships between the family history of other primary cancers and BRCA mutations. To identify factors associated with family history of other primary cancer, an ordinal logistic regression analysis was applied including BRCA mutations and risk factors for the inclusion criteria. SAS software (SAS 9.1.3; SAS Institute Inc., Cary, USA) was used for statistical analysis. Probability values less than 0.05 were considered statistically significant.
RESULTS
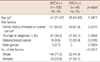
The median age of the 238 eligible patients was 41 years (range, 21-68 years). BRCA mutations were detected in 49 (20.6%) of the patients, while variants of unknown significance were detected in 13 (5.5%) patients. BRCA1 and BRCA2 mutations were detected in 23 (9.7%) and 25 (10.5%) patients, respectively. One patient, the subject of a recent case report, had mutations in both BRCA1 and BRCA2 [20]. The distributions of risk factors according to BRCA mutation status are presented in Table 1. The BRCA-positive group had a higher frequency of family history and bilateral breast cancer. There were 27 (55.1%) patients who had two or more risk factors in the BRCA-positive group, while 43 (22.8%) patients had multiple risk factors in the BRCA-negative group (p<0.0001).
There were 271 members of 156 (65.5%) families who had histories of cancer other than breast or ovary. The familial pedigree of a representative patient who had two risk factors, family history of breast cancer and younger age at diagnosis, is shown in Figure 1. There were two family members who had histories of other cancers, thyroid and uterus. The members with breast or other cancer had BRCA1 mutations revealed by genetic testing. The mother of the sibling also had the mutation.
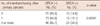
Among the 156 patients with family history of other primary cancer, 37 (23.7%) patients had BRCA mutation. It was detected in 12 (14.6%) of the 82 patients without family history (p=0.0996). Multiple cases in a single family occurred in 70 families. Among them, 24 (34.3%) were families of the BRCA-positive patients, which was significantly more frequent than expected by chi-square test (p=0.0996) (Table 2). By ordinal logistic regression, the occurrence of multiple other primary cancers was associated with BRCA mutations, not with other risk factors (Table 3).
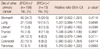
The most common site of other primary cancer was the stomach, which corresponds with research findings that stomach cancer is the most common cancer in Korea [21]. In the BRCA-positive group, the proportional incidence of uterine cancer was 12.3%, which was relatively higher than that of the BRCA-negative group (5.6%, p=0.0590) (Table 4).
DISCUSSION
In this study, we described the patterns of familial cancers other than breast or ovary of patients with high risk breast cancer. Among the 238 eligible patients, 156 (65.5%) patients had a total of 271 familial cancers. BRCA mutation was detected in 49 (20.6%) patients, which was more prevalent in patients who had family history of other primary cancers (37 patients, 23.7%, p=0.0996). Seventy patients had multiple familial cancers. BRCA mutation was also detected prevalently in patients with multiple familial cancers (24 patients, 34.3%, p=0.0034). Ordinal logistic regression analysis supported the finding that BRCA mutation was significantly associated with multiple familial cancers (p=0.0045).
The most prevalent other primary cancer was stomach cancer, which is the most common cancer in Korea [21]. According to the cancer statistics of Korea, 15.7% of all cancer was stomach cancer. In this study, stomach cancer accounted for 24.7% and 20.5% of BRCA-negative and positive group, respectively. But the difference of the proportional incidence was not statistically significant. Unlike the Korean characteristics, stomach cancer is the fourth most common malignancy in worldwide after lung, breast, and colorectal cancer [22,23]. In contrast, non-melanoma skin cancer which is relatively prevalent in Western families with BRCA mutation was rare in this study [11,24].
Pancreatic cancer showed the most distinctive difference from nationwide statistics. The proportional incidence was 6.8% and 2.4% in this study and nationwide, respectively (p=0.0137). The risk of pancreatic cancer has been known to be higher among carriers of BRCA mutations [7,8]. And pancreatic cancer has been shown to the third most common cancer associated with BRCA mutation [25]. BRCA mutations as a predisposing factor for the development of pancreatic cancer may have contributed to the results of this study [10,12]. In addition to BRCA mutations, several environmental, biological, and genetic factors might contribute to the distribution of familial cancers. It may be affected in part by the distributions of cancer nationwide, and also expected to be influenced by cancer susceptibility from the BRCA mutation.
In the Korean population, there are several distinctive features in regard to breast cancer. The first is younger age at onset of breast cancer than in other populations [26,27]. However, the incidence of BRCA mutations does not differ from that of other racial groups [19]. Although there had been no known founder mutation, the BRCA2 c.7480C>T mutation (7708C>T according to the BIC nomenclature) has been suggested as candidate for the founder mutation in Korea [18,28,29]. Several studies have dealt with BRCA mutations in Korean breast cancer patients, but they have been confined to prevalence of BRCA mutations or relationships with risk factors. In high-risk patients, the frequency of BRCA mutations varied from 8.3 to 25% according to the risk factors, which was comparable to that of this study (20.6%) [18,29]. Although the relationship between BRCA mutations and secondary malignancies was previously investigated [19], the relationship between the mutations and familial malignancies has not been studied yet in Korea. Because BRCA1/2 mutation testing in Korean population is still not common, recruitment of more family members of carriers needs to provide more information about second primary malignancies associated with in family members of BRCA mutation carriers. The Korean Hereditary Breast Cancer (KOHBRA) study, a nationwide, multicenter study is expected to provide the answer [29]. In the absence of such information, the results of our study suggest such an association from one of the biggest general hospitals in Korea that has nationwide coverage of patients.
Future directions require a focus on providing optimal genetic counseling and testing for family members. According to the National Comprehensive Cancer Network's (NCCN) guideline for genetic/familial high-risk assessment: breast and ovarian, genetic counseling is highly recommended when an individual has one or more of the following factors: early age onset breast cancer, triple negative breast cancer, two incidences of breast cancer in a single individual, male breast cancer, and personal/familial history of pancreatic cancer with familial/personal history of breast and/or ovarian cancer [30]. When the hereditary breast and/or ovarian cancer syndrome testing criteria are met, genetic testing for BRCA1/2 and screening for breast and ovarian cancer should be considered. In addition, a full body skin examination for melanoma and investigational protocols for pancreatic cancer might be considered for other cancer screening. Possible inherited cancer risk to relatives, options for risk assessment, and management should be advised.
In conclusion, BRCA mutations were associated with having multiple risk factors in patients with high risk breast cancer. In the BRCA-positive group, primary cancers of family members were found in pancreas and uterus at higher than nationwide reported incidences. Occurrence of multiple familial cancers was associated with BRCA mutation, and not with other risk factors. Tailored genetic counseling based on precise information should be provided to families with BRCA mutation carriers.


 XML Download
XML Download