

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bone metastases from breast cancer can cause skeletal complications, including bone pain, pathologic fractures, spinal cord compression, and hypercalcemia of malignancy [1]. After the initial diagnosis of bone metastasis, the median survival for breast cancer patients is approximately 18 to 26 months [2]. Furthermore, patients often need to undergo radiotherapy or surgery in order to treat bone pain or pathologic fractures; therefore, metastasis to the bone can have a significant negative effect on the quality of life of breast cancer patients.
Intravenous (IV) bisphosphonates are the standard of care for the prevention of skeletal complications in breast cancer patients with bone metastases. Zoledronic acid is a new, potent bisphosphonate that has recently been used for the treatment of patients with osteolytic lesions secondary to advanced breast cancer. The American Society of Clinical Oncology recommends the IV administration of zoledronic acid (4 mg) every 3 to 4 weeks for patients with radiologic evidence of bone destruction [3].
Bisphosphonates, including zoledronic acid, have been used to treat osteoporosis to reduce the risk of vertebral and hip fractures [4]. A recent case series report has described patients treated with alendronate, who developed atypical femoral fractures following low-energy trauma, including some with simultaneous bilateral fractures. This suggests that the risk for fractures may be increased with long-term use of bisphosphonates [5-7]. It is thought that prolonged use of bisphosphonates may lead to adynamic, fragile bone.
Patients with skeletal malignant involvement receive much higher cumulative doses of bisphosphonates than patients with osteoporosis. Atypical femur fractures have been reported after use of alendronate, but on rare occasion, there have been reports of atypical femur fractures that occurred after administration of zoledronic acid. The following case report describes a breast cancer patient with bone metastasis, in whom atypical subtrochanteric fractures developed after treatment with zoledronic acid.
CASE REPORT
A 56-year-old female with cancer in the right breast underwent a modified radical mastectomy in December 2001. At that time, the patient was diagnosed with breast cancer in stage T2N1M0. The tumor was positive for estrogen and progesterone receptors on immunohistochemical staining, and negative for HER2 overexpression by fluorescence in situ hybridization. Postoperatively, the patient was treated with adjuvant chemotherapy of cyclophosphamide, doxorubicin, and 5-FU every 3 weeks, for 6 cycles duration from December 2001 until May 2002, and hormonal therapy (toremifene citrate) from May 2002 until April 2006.
In April 2006, a follow-up bone scan revealed metastasis to the left scapula (Figure 1A), for which the patient was treated with doxorubicin and docetaxel every 3 weeks for 3 cycles. A follow-up bone scan revealed exacerbation of the metastasis, and in March 2007 (Figure 1B). At that time, the patient received intravenous (IV) zoledronic acid (4 mg) to prevent skeletal complications.
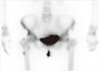
In October 2010, the patient accidentally tripped while walking and subsequently, felt pain in her right hip. Because she had no problems walking, she did not receive any specific treatment. A follow-up bone scan 1 month later demonstrated a focus of increased tracer uptake; however, the patient had no complaints of hip pain (Figure 2). The finding was thought to be a bone metastasis, and zoledronic acid was administered on an ongoing basis.
In March 2011, the patient underwent X-ray evaluation at a local clinic because of intermittent right hip pain that was negative for fracture (Figure 3). The following April, she developed pain in her right hip while jogging and had problems walking. Subsequent X-rays showed a right subtrochanteric fracture (Figure 4) and she underwent an open reduction with internal fixation (using compression hip screw & autogenous iliac bone graft) (Figure 5). A bone biopsy of the fracture site demonstrated acute and chronic inflammation.
In addition, the left femur was observed to have cortical thickening and beaking on X-ray (Figure 6). Therefore, treatment with zoledronic acid was stopped. The patient was treated with zoledronic acid from March 2007 until April 2011. Then, she was seen on routine follow-up in August 2011; the patient was using a wheel chair and the incomplete union of her right subtrochanteric fracture remained.
DISCUSSION
The results of several studies have indicated that bisphosphonates are very useful in the treatment of osteoporosis and malignant involvement of the bony skeleton. This class of medications reduces the risk of skeletal-related events, as well as both vertebral and nonvertebral fractures [8-11]. However, there have been several case series describing patients administered bisphosphonates over a long period that developed "atypical" subtrochanteric (defined as within 5 cm distal to the lesser trochanter of the femur) and diaphyseal fractures of the femoral shaft. This suggests that there may be increased risk for fractures with long-term use of bisphosphonates [5-7].
Neviaser et al. [5] described a type of fracture of the femoral shaft that is specific for patients being treated with bisphosphonates. The fracture occurs after minimal or no trauma, and is characterized by 1) a simple, transverse pattern, 2) unicortical beaking, and 3) hypertrophied diaphyseal cortices. Awareness of this type of fracture is very useful for recognition of the pathogenesis of the fracture. The proximal femoral shaft is subjected to high stresses and would not be expected to fracture after minimal trauma without underlying metabolic bone pathology, such as osteoporosis. Our patient developed a transverse fracture with cortical beaking after minimal trauma. In addition, subtrochanteric stress fractures are uncommon and occurred in isolated cases, such as hypophosphatemic osteomalacia [12,13].
Atypical fractures associated with long-term use of bisphosphonates have been seen in patients with osteoporosis, who were treated with alendronate. Odvina et al. [6] reported on 9 patients who had sustained, spontaneous nontraumatic fractures while receiving prolonged alendronate therapy. Furthermore, Goh et al. [7] reported on 13 subtrochanteric fractures that occurred over a 10-month period, 9 of these fractures were in patients being treated with alendronate. However, atypical subtrochanteric fractures have been rarely reported in breast cancer patients with bone metastasis who were treated with IV zoledronic acid.
Patients with skeletal malignant involvement receive much higher cumulative doses of bisphosphonates than patients with osteoporosis, and may be at higher risk for the development of these atypical femoral fractures. Puhaindran et al. [14] reported that 4 of 327 cancer patients with bone metastasis or myeloma, who were treated with IV zoledronic acid or pamidronate, developed atypical subtrochanteric femoral fractures. They concluded that the prevalence of atypical subtrochanteric femoral fractures in patients with skeletal malignant involvement, who were managed with high doses of intravenous bisphosphonates was low.
Many authors have asserted that complications or nonunion are most likely to occur in insufficiency fractures of patients treated with long-term bisphosphonates. Odvina et al. [6] reported that 6 of 9 patients with spontaneous nonspinal fractures manifested delayed or absent healing of their fractures while undergoing long-term alendronate therapy. The patients described that the nonspinal fractures healed poorly, while the patients were on aledonate, but healed satisfactorily after treatment in most patients. Four months after undergoing internal fixation of her fracture, our patient also manifested delayed union.
IV zoledronic acid is an effective and safe treatment for the prevention of the skeletal complications in breast cancer patients with bone metastasis, and there have been rarely reports of atypical fractures occurring in patients treated with zoledronic acid. Black et al. [15] reported a large randomized trial of zoledronic acid, which was no significant increase in risk associated with zoledronic acid. However, because of limitation of a small number of events, the study underpowered for definite conclusion. However, if a fracture occurs, the patient may require surgery and rehabilitation, and there may be delayed union of the fracture. Therefore, administration of zoledronic acid must be undertaken with care, and based on our experience; both doctors and patients should keep in mind the possible occurrence of atypical subtrochanteric fracture. In addition, routine X-rays should be undertaken to investigate any signs and symptoms associated with atypical fractures that occur in breast cancer patients with bone metastasis.





 XML Download
XML Download