

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cyclophosphamide is an alkylating agent commonly used in antineoplastic and immunosuppressive therapies. Its side effects when used in high doses include bone marrow depression, alopecia, mucositis, sterility, hemorrhagic cystitis, and symptomatic hyponatremia due to severe water intoxication [1,2].
Severe hyponatremia (serum sodium<120 mmol/L) is a serious electrolyte disorder with life-threatening neurological complications and is rarely induced by low dose cyclophosphamide (<20 mg/kg). Until now, there has been only one reported case of severe hyponatremia with generalized seizure from low-dose intravenous cyclophosphamide based chemotherapy in a breast cancer patient [3]. We report a case of severe, symptomatic hyponatremia that developed in a female breast cancer patient following the first cycle of chemotherapy containing low-dose cyclophosphamide.
CASE REPORT
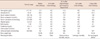
A 56-year-old woman was scheduled to receive four cycles of adjuvant chemotherapy containing doxorubicin 60 mg/m2 and, cyclophosphamide 600 mg/m2 (AC) and thereafter four cycles of adjuvant chemotherapy containing paclitaxel 175 mg/m2 (T) with a three-week time interval for stage IIB (pT2N1M0) invasive ductal carcinoma of the right breast. Her past medical history included hypertension and cerebral hemorrhage in the left temporal lobe that developed 15 years prior, for which she was treated properly with propranolol 40 mg, nifedipine 30 mg, enalapril maleate 10 mg, and acetyl salicylic acid 100 mg once daily without experiencing any side effects. Her laboratory tests and 2-D echocardiogram were normal before the first cycle of adjuvant chemotherapy. During the first cycle of adjuvant chemotherapy containing doxorubicin 90 mg and cyclophosphamide 900 mg, she was hydrated with 1.0 L of isotonic saline and received antiemetic therapy consisting of dexamethasone and palonosetron. She was discharged the following day without any immediate side effects of the chemotherapy. Her serum electrolyte level was not routinely checked prior to discharge. She went to the emergency department the following day (50 hours after adjuvant chemotherapy) due to general weakness, nausea, vomiting, and edema. Just after arriving at the hospital, she developed a generalized seizure with convulsions, following a period of impaired consciousness and incoherent speech. A Glasgow Coma Score of 3 was noted. Her vital signs were blood pressure 140/80 mmHg, pulse rate 78 beats/min, and body temperature 37.1℃. Laboratory tests showed the followings: hemoglobin 14.2 g/dL, platelets 201,000/mm3, white blood cell count 7,800/mm3, blood urea nitrogen 8.2 mg/dL, serum creatinine 0.65 mg/dL, serum sodium concentration 116 mmol/L, serum potassium 3.6 mmol/L, serum chloride 87 mmol/L, serum albumin 4.3 g/dL, serum osmolality 254 mOsmol/kg, and urine sodium concentration 34 mmol/L. Urine analysis showed specific gravity 1.039, pH 6.5, protein -, blood -, WBC/high powered field (HPF) 0-1, red blood cells/HPF 0-1. The brain computed tomography (CT) revealed no interval change as compared to the previous brain CT. To correct her severe symptomatic hyponatremia, urgent medical treatment with hypertonic saline solution and furosemide was initiated carefully. Within 12 hours, her serum sodium concentration rose gradually from 116 to 126 mmol/L and the patient slowly recovered from her neurological symptoms. The serum sodium concentration was gradually corrected to 136 mmol/L by infusion of isotonic saline for the next two days (Table 1). She was discharged asymptomatically after 10 days and was admitted to the hospital for the second adjuvant chemotherapy. She was treated with 20% dose reduction of chemotherapy and we checked her body weight, electrolytes, and input/output daily to prevent severe hyponatremia induced by low dose cyclophosphamide. Although she had water retention with a 2 kg-weight gain during the chemotherapy, she was successfully treated with hypertonic saline solution and furosemide without any neurologic symptoms. We will treat her with adjuvant AC (doxorubicin + cyclophosphamide) chemotherapy as initially scheduled.
DISCUSSION
Symptomatic hyponatremia with a generalized seizure was observed in our patient 48 hours after treatment of the first cycle of AC chemotherapy. Hyponatremia usually occurs 4-12 hours after the administration of cyclophosphamide, although sometimes not until 48 hours afterwards, as in our case, and returns to normal in around 24 hours. The antidiuretic effect seems to be related to the appearance of active alkylating metabolites of cyclophosphamide [4].
We suspected intravenous low-dose cyclophosphamide-based chemotherapy as the cause of severe hyponatremia since other causes were ruled out. She had been diagnosed with cerebral hemorrhage with hypertension in 1996. A cerebral hemorrhage lesion in her past medical history could have caused a generalized seizure with convulsions, but her brain CT and magnetic resonance imaging scan showed no interval changes before and after the seizure attack, and she recovered from her neurologic symptoms after the correction of her hyponatremia. The enalapril maleate that she took as an antihypertensive drug could also have caused hyponatremia. However, she had been well, without any symptoms related to hyponatremia during the treatment of hypertension with enalapril maleate. However, it is necessary to keep in mind the possibility that her past medical history, including the cerebral hemorrhage and enalapril maleate medication, may have been predisposing factors that deteriorated her severe hyponatremic symptoms.
In this case, she had a 3.5 kg-weight gain after chemotherapy. Although we performed overhydration on her to prevent hemorrhagic cystitis, this was not enough to explain her weight gain and severe hyponatremia. After her discharge from the hospital, she insisted on a low salt diet due to her concern about hypertension. Water intoxication induced by low-dose cyclophosphamide might have been accelerated due to overhydration and her low salt diet.
Severe hyponatremia has been previously reported in patients treated with high-dose cyclophosphamide (30-40 mg/kg) and moderate-dose (20-30 mg/kg) intravenous cyclophosphamide [5-9]. There have been four malignant disease cases in which severe symptomatic hyponatremia was reported from low-dose intravenous cyclophosphamide therapy including, our case and other malignant disease cases [3,10]. Two cases, including our case, were women with breast cancer suffering from severe hyponatremia after adjuvant chemotherapy, and another was a man with multiple myeloma suffering from severe hyponatremia after a single dose of low-dose cyclophosphamide. The last one was a woman with metastatic adenocarcinoma of small salivary glands who received a cycle of AC chemotherapy and concomitant use of cisplatin [11]. Those data are summarized in Table 2.
The mechanisms of hyponatremia induced by cyclophosphamide have not been clearly understood, but there are some possible mechanisms of cyclophosphamide induced hyponatremia. Harlow et al. [6] suggested a syndrome of inappropriate antidiuretic hormone secretion. That hypothesis is corroborated by the postmortem examination that was performed on one patient who received high-dose cyclophosphamide, and demonstrated loss of Herring's bodies and degranulation of various hypothalamic neurosecretory organelles. The cyclophosphamide metabolite could act indirectly by causing ADH release; this has been demonstrated with ifosfamide, a close structural analogue to cyclophosphamide. Lee et al. [12] speculated that the antidiuretic effect of cyclophosphamide might be related to increased renal action of vasopressin by alkylating metabolites, and water retention might involve a direct tubular effect of cyclophosphamide metabolite on the collecting duct epithelium, because it was demonstrated in a case with established diabetes insipidus that developed cyclophosphamide associated antidiuresis without vasopressin secretion [13]. Therefore, further studies will be necessary to evaluate the molecular mechanisms of hyponatremia induced by cyclophosphamide and establish dose dependant relationships of cyclophosphamide with the severity of hyponatremia.
We have learned many lessons from this case. First, overhydration and hypotonic saline solution use should be avoided in prechemotherapy hydration. Second, common symptoms like nausea, vomiting, and general weakness due to chemotherapy might be a sign of severe hyponatremia. Third, clinicians must pay more attention to a patient with comorbidities such as nephritic syndrome or concurrent medications that can be associated with hyponatremia.
In conclusion, clinicians must always keep in mind that life-threatening acute hyponatremia can be induced by intravenous cyclophosphamide during chemotherapy, even if the dosage is low.

 XML Download
XML Download