

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sentinel lymph node biopsy (SLNB) has become the standard method for axillary staging of breast cancer with reliable accuracy and fewer morbidities compared to complete axillary lymph node dissection (ALND) [1-3]. A sentinel lymph node (SLN) is defined as one of the first nodes to receive lymphatic drainage from a tumor bed [4,5]. However, there may be more than one SLN in an axillary bed [6,7], and the SLN is now defined as any lymph node or first set of nodes that receives direct lymphatic drainage from a primary tumor [8,9].
The mean number of SLNs removed ranges from 1.2 to 3.4, with the total number ranging from 1 to 8 [7,10-14]. Faced with multiple SLNs during the SLNB procedure, one of the primary issues is how many SLNs should be removed. This question needs to be answered, because the number of SLNs removed is significantly associated with an increased incidence of axillary complications [15].
To date, the optimal number of SLNs that should be removed to accurately predict axillary lymph node status remains controversial. We hypothesized that there might be an optimal threshold number of SLNs to be removed to achieve acceptable accuracy. The aim of this study was to determine the appropriate number of SLNs to be removed for accurate axillary staging with minimal morbidity.
METHODS
Between January 2004 and December 2005, 328 patients with clinically node negative invasive breast cancer, who underwent SLNB followed by complete levels I and II ANLD at Severance Hospital, Yonsei University College of Medicine in Seoul, Korea were enrolled. We excluded patients who had neoadjuvant chemotherapy, previous axillary surgery or radiation, and those who did not consent to scheduled surgical procedures. Patients who only underwent a SLNB or in whom we could not detect SLNs were also excluded. The information regarding SLN characteristics (number and order of SLNs) and pathological findings (SLNs and non-sentinel lymph nodes) were prospectively recorded in the Severance Hospital Breast Cancer Registry.
SLN detection was only performed using the radio-isotope technique. On the day of surgery, 18.5 MBq (0.5 mCi) 99mTc Phytate (Korea Atomic Energy Research Institute, Daejeon, Korea) diluted in 0.5 mL saline was injected using the subareolar technique. A lymphoscintigraphy was performed after injection. The incision was made over the hottest area identified using a handheld probe (Navigator GPS; RMD Inc., Watertown, USA). After opening the axillary fascia, a handheld gamma probe was inserted to detect areas of concentrated hot nodes and to guide the ANLD. SLNs were judged as any node with radioactive counts 10% or more of the ex vivo count of the most radioactive SLN. After the SLNB, all patients received planned level I/II ANLD by two experienced breast surgeon regardless of SLN status to validate our early experience with SLNB.
SLNs <1 cm were cut into two blocks, and two serial sections were taken from one block for the frozen sections, whereas another block was subsequently converted to paraffin sections. Intraoperatively frozen sections were stained with hematoxylin and eosin (H&E). The remaining frozen specimens and all non-sentinel nodes underwent a routine pathological evaluation using H&E with or without immunohistochemical staining for cytokeratin. Patients with metastases detected by any method were considered positive for metastatic disease. Isolated tumor cells measuring <0.2 mm were classified as N0 disease. The false negative rate was defined as the proportion of patients with negative SLN findings on frozen or permanent sections who were subsequently found to have disease in the axillary lymph nodes on ALND. Accuracy is the proportion of all patients (positive or negative findings of sentinel lymph node biopsy) for whom the SNB correctly predicted the ALND results. The false negative rate (FNR) and accuracy of SLNB were evaluated according to the number of removed SLNs.
RESULTS
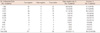
The patient clinicopathological characteristics are summarized in Table 1. The mean age of the patients was 48.1 years (range, 24-79 years). In total, 216 (65.9%) patients underwent a total mastectomy, and 112 (34.1%) received breast conservation therapy. The primary tumor classification was 210 patients (64.0%) with T1 and 118 patients (36.0%) with T2. Invasive ductal carcinoma was the most common histological tumor type (323/328, 98.5%). There were four (1.2%) invasive lobular carcinomas and one (0.3%) other cancer.
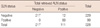
The number of SLNs identified at the time of surgery ranged from 1 to 14 (mean, 3.0±2.1). The mean number of retrieved axillary nodes examined was 17.5±5.9 (range, 10-40). Pathologically positive axillary lymph nodes were identified in 111 (33.8%) patients (Table 1). Of patients with negative SLNs, 12 patients had positive non-sentinel axillary lymph nodes yielding a FNR of 10.8% (12/111) and the overall accuracy of SLNB in our series was 96.3% (316/328) (Table 2).
Clinicopathological characteristics of the 111 patients with positive axillary lymph nodes were compared with 12 cases of false negative patients and 99 cases of true positive using the chi-square test. No differences in age distribution, tumor size, estrogen receptor status, or histological grade were observed (data not shown).
There were five cases of isolated tumor cells, pN0[i+], seven cases of pN1mi, and five cases of macrometastasis in which the frozen SLN sections were negative but permanent sections were positive. Therefore, 12 (3.7%) false negative cases were found during the freezing process, and these were not considered false negative results.
The number of SLNs removed and the corresponding number of patients are summarized in Table 2. Ninety-two patients (28.0%) had one SLN removed, 82 patients (25.0%) had two SLNs removed, 57 patients (17.3%) had three SLNs removed, and 32 patients (9.7%) had four SLNs removed. More than four SLNs were removed in 65 patients (19.8%). The FNR was 26.6% (8/30) for single SLN removal, 8.0% (2/25) for two SLNs, and 11.1% (2/18) for three. When four SLNs were removed, the FNR was 0% (0/14). The accuracy of SLNB was 91.3% (84/92) for single SLN removal, 97.6% (80/82) for two, and 96.5% (55/57) for three. When four SLNs were removed, the accuracy was 100%, and removing more than four SLNs did not improve the accuracy of axillary staging any further (Table 2). The FNR and accuracy according to the number of SLNs removed are summarized in Table 3. The overall pathological status of SLN and axillary lymph nodes are summarized in Table 4. The accuracy of SLNB was 100% with 0% FNR when four or more SLNs were removed.
DISCUSSION
SLNB has replaced ALND as the stand-alone axillary staging procedure for patients with clinically node negative breast cancer. The NSABP B-32 trial, the largest multicenter trial to date for the evaluation of SLNB, confirmed that overall survival, disease-free survival, and regional control were equivalent between an SLNB alone group and a SLNB with axillary dissection group [16].
A SLN is defined as the first node to receive lymphatic drainage from a primary tumor bed [4,5]; however, the actual experience of most investigators includes more than one SLN and controversy still exists regarding the optimal number of radioactive SLNs that should be removed to ensure accuracy and minimize morbidity [6,7].
One of the possible explanations for identifying multiple SLNs is the "pass-through" phenomenon, which reflects isotope migration from the "true" SLN into secondary echelon lymph nodes. Another simple explanation is normal anatomical variation in which the lymphatics of a given site simultaneously drain into more than one SLN [7].
A benefit of SLNB is that it removes fewer nodes compared with standard ALND, thereby reducing morbidity. The key factor used to assess the success of SLNB is the FNR because it defines the frequency of negative SLNs when other axillary nodes have metastases. So, an acceptable accuracy of axillary staging must be determined to minimize SLNB-related morbidity.
How many sentinel nodes should be removed to achieve appropriate accuracy of axillary staging without negating the potential benefits of SLNB? We hypothesized that there is a point when the surgeon can terminate the procedure without sacrificing SLNB accuracy. In our series, 100% of positive SLNs were identified in one of the first three lymph nodes removed in patients with node positive disease. Furthermore, 100% accuracy of SLNB was achieved by excising four nodes but removing all SLNs with radioactive counts >10% of the ex vivo counts of the hottest SLN did not increase accuracy.
Our data are quite comparable to the majority of published series that have evaluated the optimal number of SLNs and support the trend of limiting SLN biopsy to 3-4 lymph nodes. Although no clear data exist regarding limiting axillary dissection based on relative radioactive counts, limiting SLNB to a reasonable number of nodes, about 3 or 4, is well supported by several case series, including this report. Published data show that 97-98% of positive SLNs are discovered in one of the first three nodes examined, and that it is rare to find a positive SLN after identifying the first three nodes as negative [6,7,14,17-20]. Some recent data also demonstrate that >98% of positive SLNs are identified in one of the first four lymph nodes removed [21]. These data demonstrate that the total number of SLNs to be excised can be limited to four without jeopardizing the accuracy of axillary staging. We suggest that the SLN should be among the hot nodes if all hot nodes are removed, but not all hot nodes are SLNs.
In 2001, McCarter et al. [7], suggested that there is no absolute upper threshold for the number of SLNs that should be removed. However, indiscriminate removal of axillary nodes may not be justified, considering operative complications and resource utilization associated with SLNB. Data from the ACOSOG Z0010 prospective trial comparing SLNB only with SLNB followed by complete ALND found an increase in the rate of axillary seroma formation and wound infections in patients who had more than four SLNs removed [15]. Furthermore, cost-effectiveness and cost utilization studies have found that excising a high number of SLNs is associated with longer operation time, higher pathology costs, and higher procedural costs [22]. Terminating the procedure after the fourth node may lower the cost of the procedure and reduce morbidity.
Our data also suggest that removing only a single SLN increased the risk for FNR. In our series, FNR was 26.6% for a single SLN removed, which is outside the acceptable FNR range of 5-10% [23-25]. It has been established that the SLN with the highest radioactive counts is not always the SLN that is most likely to harbor metastatic disease [26,27]. Why is an SLN not necessarily the "hottest" node in the lymphatic basin? We can offer three reasons for this. First, when the radioactive tracer passes through an SLN, if the next lymph node stage is relatively large or if there are active phagocytic cells, more radioactivity material is accumulated than in the first lymph node stage. Second, the amount of radioactive tracer accumulated in a lymph node not only depends on the order of drainage but also reflects the number of lymphatic channels and lymphatic flow. Last, if a true SLN is occupied by metastatic cells, it cannot absorb radioactive tracer. In that case, another lymph node will ingest tracer and be recognized as an SLN. Therefore, we cannot say that the so-called "hottest node," which absorbs the most radioactive tracer, is always the first SLN [28,29]. In this respect, to find the SLNs in a case of fewer than four hot nodes should be a very important line of research in the near future.
Limitation of the present study was a different proportion of operation methods compared to the nationwide Korean Breast Cancer Society (KBCS) registration program. Ko and the KBCS [30] reported that approximately 50-55% of whole breast cancer patients including in situ carcinoma and metastatic disease underwent total mastectomy during same study period. Since type of surgery is determined not only by tumor size but also by various clinicopathological parameters, radiological findings, or a patient's desire, our present results using selected study cohort at single institution remain to validated in an independent dataset.
In conclusion, excising all SLNs with >10% of the counts of the hottest SLN could result in oversampling. We suggest that the total number of SLNs excised be limited to no more than four. We also suggest that the SLNB is not complete by removing only one or two nodes or only the hottest node. By removing only the nodes most likely to contain metastases, the SLN procedure potentially avoids complications commonly described for ALND without compromising staging.


 XML Download
XML Download