

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the second most common cancer among women in Korea. Crude incidence rate of breast cancer is 47.4 per 100,000 women and 11,606 new cases were diagnosed in 2007. In the Western countries, the most significant factor of all risk factors for contracting breast cancer is age. However, it is not the case in Korea. More than fifty percent of all cases occur in women under 50 years of age. The prevalence in terms of age is the highest in 40s (39.7%), followed by 50s (24.98%) and 30s (14.80%). Also the 5-year relative survival rate has risen from 77.9% between 1993 and 1995 to 89.5% between 2003 and 2007 [1]. Considering high proportion of premenopausal patients and increasing 5-year relative survival rate, more younger patients are becoming long-term survivors and the quality of life (QOL) issue becomes crucial.
Many factors have been identified as related to QOL of breast cancer survivors, and younger age has been known to be one of the significant high risk factors for poor quality of life [2-6]. Previous studies suggest that younger women have greater psychological morbidity and poorer QOL after breast cancer diagnosis than older women [2,5,7-9]. However, the relationship between age and psychosocial adjustment has not been consistent in other studies of breast cancer patients [10-13]. Mosher and Danoff-Burg [14] reviewed studies on age differences in psychological adjustment to breast cancer and suggested age may be best viewed as a risk factor for distress with other variables operating to produce this demographic difference, but more studies be needed to clarify the mechanism underlying age difference in adjustment.
Although the incidence of breast cancer is rapidly increasing, few studies have addressed quality of life among breast cancer survivors and moreover, no research has been performed on age-related QOL in Korea. In order to provide age appropriate psychosocial services, it is necessary to find age-related QOL differences and to examine the unique effect of age on QOL.
Thus, the aims of present study are threefold: to examine if there are QOL differences between younger and older breast cancer survivors; to identify age-correlated variables affecting QOL; and to determine the unique effect of age on QOL among breast cancer survivors.
METHODS
Patients and procedures
All participants were outpatients at Yonsei University Severance Hospital Breast Cancer Clinic who were attending follow-up medical appointments after surgery. The study was approved by the Institutional Review Board. Eligibility criteria for this study were 1) between 20 and 80 years old, 2) stage I, II, and IIIB, 3) no evidence of systemic metastasis, 4) no evidence of psychosis, dementia, or suicidal behavior, and 5) those who agreed to participate in this study. Patients were approached in the waiting area before their appointment, at which time the study was briefly described, and they were asked to participate. Written consent was obtained from all the participants prior to administering the tool. Participants completed questionnaires in the waiting area and returned the questionnaire at the end of their appointment. The study coordinator was available to answer any questions. One thousand two hundred fifty eligible subjects participated in the study and 1,094 cases were used for analysis as appropriate. Patients were divided into two groups in this study: women age <50 years and women age ≥50 years. Age was dichotomized as <50 years and ≥50 years to serve as an approximate indicator of menopausal status. This cutoff point is used in epidemiologic literature [15] and large breast cancer QOL studies [4,16] as well as clinical practice.
Measures
Socio-demographic and clinical backgrounds
Socio-demographic variables such as age, current marital status, job, education, and economic status were included in the survey. The medical/treatment variables were collected by reviewing the patients' medical records. The question about level of daily activity was also included in the survey.
Functional Assessment of Cancer Therapy-Breast cancer
The Functional Assessment of Cancer Therapy-Breast cancer (FACT-B) version 4 was used to assess health-related QOL. The FACT-B is a 36-item questionnaire that measures both the 27-item general QOL associated with cancer (FACT-G) and the additional 9-item breast cancer related QOL, breast cancer subscale (BCS). FACT-B consists of the following subscales: physical well-being (PWB), functional well-being (FWB), emotional well-being (EWB), social/family well-being (SWB), and BCS. The psychometric properties of the FACT-B are well documented [17], and it was validated in Korean [18]. The test was administered and scored in accordance with the instructions of the version 4 provided by the Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System (www.facit.org). A total FACT-B score is calculated by summing the subscales. The instrument asks respondents to rate how true each statement is for the last 7 days. Response scales range from 0 (not at all) to 4 (very much). Cronbach α was 0.79-0.90 in the Korean version of FACT-B [18], and Cronbach α in this study was 0.915 for the total FACT-B, 0.855 for PWB, 0.867 for SWB, 0.807 for EWB, 0.904 for FWB, and 0.681 for BCS.
Global QOL
The global QOL using a single-item measure called the Ladder of Life was used to assess the subjective QOL. The study participants are asked to circle the number that represents how they feel at the present time. One represents the worst possible and 10 represents the best possible life. It has been shown to be good summary measures of QOL [19].
Statistical methods
Descriptive statistics were used to analyze demographic and clinical characteristics of the sample. Age-related differences in QOL between two groups were ascertained with t-test. Chi-square was conducted to identify age-correlated variables. We conducted a series of multiple regression analyses to evaluate the unique contribution of age variable on QOL of breast cancer patients after adjusting age-correlated variables. Age was considered as both a continuous and dichotomous variable. However, the results were similar, only the results for the dichotomous analysis were reported. Data analyses were conducted using the SPSS version 17.0 (SPSS Inc., Chicago, USA). A p less than 0.05 was considered statistically significant.
RESULTS
Age differences in socio-demographic and clinical variables
The socio-demographic and clinical characteristics of the two groups are shown in Table 1. The mean age was 46.9 years and women age <50 years were 65.4 percent.
In this sample, significant socio-demographic and clinical differences existed based on age categories. Women age <50 years reported higher educational levels (p<0.001), more being employed (p<0.001), more likely to have received chemotherapy (p<0.05), and significantly higher levels of daily activity (p<0.001) than those age ≥50 years. Also, women age <50 years were more likely to have been longer time since surgery than older counterparts (p<0.01). There were no age-related differences in operation method, radiotherapy or hormone therapy received.
Quality of life differences by age group
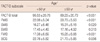
The results of t-test demonstrated strong age effects on QOL (Table 2). Younger women (age <50 years) showed significantly higher QOL scores than older women (age ≥50 years) in all of the QOL subscales except EWB. PWB (p<0.001), SWB (p<0.05), FWB (p<0.001), BCS (p<0.01), and FACT-B Total (p<0.001) were significantly related with age. Subjective QOL measured by the Ladder of Life was also significantly related with age (p<0.01).
As shown in Table 3, in order to more specifically examine which items in breast specific concerns were correlated with age, we compared the mean scores of the respective FACT-BCS item between two age groups. The mean scores of B4 were the lowest among 9 BCS items in both age groups. Older women showed significantly worse scores in B4 (p<0.001), B5 (p<0.05), and B9 (p<0.001) than younger women. Since all the other items except B4 and B9 were reversely coded, we could consider older patients group were more likely to have worse QOL in breast cancer specific concerns, especially in those items related with sexuality than younger patients.
Differentiating effects of age from other age-correlated variables
In order to differentiate effects of age from other age-correlated variables, we conducted a series of multiple regression analyses. At first, we identified those variables that were found to significantly affect QOL of breast cancer patients. Education, job, economic status, time since surgery, operation method, chemotherapy, and daily activity were the identified predictors for QOL in our previous study [20]. Then, we examined which variables showed significant relationship to age in chi-square test as shown in Table 1. In the multivariate model, we included only those variables that were found to significantly affect QOL and showed significant relationship to age in chi-square test at the same time, in order to differentiate effects of age from other age-correlated variables. So the variables were excluded if they did not show significant relationship to age, even if they were identified to significantly affect QOL. Therefore, job, education, time since surgery, chemotherapy and the level of daily activity were identified as such variables. Finally, in order to adjust potential confounding effects of age-correlated variables affecting QOL, demographic factors such as job and education were entered first, then clinical variables including time since surgery and chemotherapy were entered and the level of daily activity was entered lastly. The unique effect of age on QOL was examined by the changes of partial coefficient and level of significance in four regression models. Table 4 presents the results of the regression models with change statistics in each step.
In model 1, the bivariate correlation between age and QOL was β=0.143 (p<0.001). Significant age effect on QOL was still observed after controlling demographic variables in model 2 (p<0.05) but the partial coefficient of age was decreased substantially after controlling job and education (β=0.075). This result indicates that QOL variance among age groups (model 1) is partially explained by the difference of age-related socio-demographic variables between two age groups.
However, the partial coefficient of age variable slightly increased in model 3 (p<0.05) after controlling additional clinical variables including time since surgery and chemotherapy. Chemotherapy and shorter time since surgery are known to be risk factors for QOL. Younger women were more likely to have received chemotherapy and to have been longer time since surgery in this study sample. Because the effect of chemotherapy was found to be stronger than time since surgery, the QOL of younger women slightly increased.
Lastly, after daily activity variable being controlled, the coefficient of age variable was diminished from β=0.077 to β=0.027 (model 4, p<0.05) and the effect of age became no longer significant in model 4. These results show that age alone does not predict QOL and age-related differences in QOL were caused by the differences of age-correlated variables such as educational level, job status, time since surgery and daily activity between two age groups.
DISCUSSION
This study examined the age-related differences of QOL between younger and older breast cancer survivors as well as the unique contribution of age after controlling for other age-correlated variables. Results from these analyses suggest that women age <50 years manifest significantly better QOL than women age ≥50 years with breast cancer in terms of the Ladder of Life, FACT-B total and all the FACT-B subscales except EWB. However, when we controlled for age-related variables in a series of regression analyses, the effect of age was no longer significant.
In this study, younger breast cancer survivors showed better QOL than older survivors in most of the QOL domains except emotional well-being. Previous studies have suggested that older age is related positively to overall QOL [2-6], which was not supported in our study. Our results were rather similar to a Japanese study [21], which reported younger patients and those with higher educational background demonstrated significantly better FACT-SWB scores.
In the Western studies, older age are known to be associated with better adjustment after surgery. They explained the age-related differences from several aspects, including more aggressive treatment being received for younger patients, emotional maturity of older patients, more resources or skills to cope with breast cancer and relative economic stability among older patient groups [3,6]. However, although younger breast cancer survivors were more likely to have chemotherapy than older groups in our study sample, younger breast cancer survivors showed better QOL than older groups. It is not sure if this result is related to the differences in the peak age of onset between Asia and the West. In a recent study, the peak age of onset in Asia is found to be 45-50 years of age, whereas it is 55-60 years in the West [22]. Also, we have national health insurance system in Korea whereas health and social policies are more available to older patients than younger patients in the United Sates [5]. So younger patients could have better accessibility to health care system and this could enhance QOL of younger patients group in Korea. However, this explanation should be provided with discretion and needs another study. More research is needed to investigate whether QOL differences result from clinical, cultural differences, or other mediating effect of age-related variables such as education.
It is important to note that older breast cancer survivors demonstrated significantly worse QOL not only in physical and functional wellbeing but even in social/family wellbeing and breast cancer specific concerns. On the subscale emotional wellbeing, younger women reported slightly higher scores than older women, although they were not statistically significant. Contrary to our study results, Kwan et al. [2] reported older age of breast cancer was related to higher scores in all QOL domains except for social/family wellbeing. In another study, there were a consistent pattern of higher QOL ratings among older women (>50 years) and statistically significant differences for emotional wellbeing and breast carcinoma specific concerns were existed [3]. On the other hand, in a study with Korean sample by Ahn et al. [23], breast cancer survivors reported better social and emotional functioning but poorer physical and sexual functioning with increasing age. Even if we suppose physical and functional wellbeing could get worse with increasing age, social/family wellbeing, emotional wellbeing and breast cancer specific concerns would not. Low scores in SWB mean that older women were less likely to receive support from spouse, family or friend than younger women. Considering that younger women were more likely to have received chemotherapy, we expected younger women would report lower scores in BCS than older women because of side effects of chemotherapy. However, it is quite surprising that older women reported worse QOL scores in several BCS items including hair loss, sexual attractiveness and feeling like a woman. These results mean older breast cancer survivors could be experiencing more breast cancer specific concerns but provided less understanding and support from family or friends. It suggests more supportive services be targeted toward older age group. Specific strategies might include organizing social support from family, friends or support group and counseling for enhancing positive self-image as a woman. Also, more concern should be given to physical and functional aspects of older patients after surgery.
Socioeconomic status and education have been known to be significantly associated with QOL and depression [21,24-28]. As shown in chi-square test, women age <50 years were more likely to have higher educational levels and more being employed, which contribute to better access to information and resources for problem solving as well as better coping skills, which might explain better QOL among women age <50 years. Providing education and information about breast cancer and its management, and linking resource might be helpful to improve QOL among older patients.
When we corrected for age-correlated variables, the unique effect of age was no longer significant in the final regression model, which confirms a previous study [29]. This means the age differences between women age <50 years and age ≥50 years were caused by the age-related variables and not by the unique effect of age. We could consider younger age group were significantly more likely to have higher educational level, more jobs, higher level of daily activity and had been for longer time since surgery than older age group and these factors contributed to age effect on QOL.
Although the unique effect of age was not found after correcting age-related variables, age-related differences in QOL between younger and older breast cancer survivors still exist. Older age group ≥50 years appear to be at high risk of overall QOL including physical, functional, social, and sexual morbidity after surgery. Those morbidities, if left untreated, are reported to lead to a disabling and prolonged illness [30].
This study has some limitations. Cross-sectional design and a convenience sample in a university hospital were used in this study. Therefore, the results should not be generalized beyond the sample of the study and should be interpreted cautiously.
In spite of its limitations, our study results showed that significant QOL differences between younger and older breast cancer patients exist but they did not result from the unique effect of age but from other age-related factors. Therefore, this study suggest those factors should be considered including lower education level, not being employed, shorter time since surgery, and lower level of daily activity as well as older age in targeting high risk patients. For effective management of limited resources, specific and age-appropriate interventions might need to be designed, such as organizing educational support groups which provide peer support, education and information about their illness, exercises and diet, etc. Preparing older women for the social, physical, function and treatment-related effects of breast cancer or involving partners and families in patient consultation may be helpful.
In conclusion, this research suggests that older breast cancer patients have more difficulty adjusting to breast cancer than younger women after surgery but age alone does not explain the differences between younger and older breast cancer survivors.



 XML Download
XML Download