

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Despite progress in early detection and treatment of breast cancer, and advances in our understanding of cancer's molecular basis, breast cancer remains a major cause of death in women.(1) Effective treatment of estrogen receptor (ER) positive breast cancer with anti-estrogenic drugs, such as tamoxifen, is well established. However, breast carcinomas eventually become refractory to hormone therapy.(2) To overcome this limitation on anti-estrogenic therapy, new therapies that selectively target specific molecules playing important roles in cancer growth or progression have been developed. As a result, there has been much success with the erbB-2 targeting agent trastuzumab which was first approved for the treatment of advanced breast cancer in 1998. Subsequently, various molecular regulators of signaling transduction pathways in tumor cells have been under investigation. Among these potential targets, there has been particular interest in several components of the phosphatidylinositol 3-kinase (PI3K)/Akt/mammalian target of rapamycin (mTOR) signaling pathway.
The PI3K/Akt/mTOR signaling pathway is an important regulator of cell growth, proliferation and survival.(3,4) Dysregulation of this pathway generates an oncogenic environment, and leads to uncontrolled proliferation of transformed clones.(5) The Akt protein, also known as protein kinase B (PKB), lies downstream of PI3k and upstream of mTOR and is implicated in various cellular processes, including cell growth, proliferation, apoptosis and regulation of gene expression.(6) The mTOR pathway is involved in regulating many aspects of cell growth and proliferation at the translational level.(6,7) Regulation is achieved by two downstream components of mTOR, 1) ribosomal p70 S6 kinase (S6K1) and 2) eukaryotic translation initiation factor 4E (eIF4E)-binding protein 1 (4E-BP1). Activation of S6K1 and eIF4E by mTOR initiates the translation of mRNAs and subsequent increased protein synthesis essential for cell growth and proliferation.(3,8)
Recently, many studies have demonstrated that there are several mutations both upstream and downstream of the mTOR kinase in malignant tumors, mutations that play an important role in the development and growth of various tumors.(3,5) These mutations include/are involved in amplification of a catalytic subunit of PI3K, loss of PTEN (phosphatase and tensin homolog deleted on chromosome 10), a tumor-suppressor gene which downregulates expression of either PI3K or Akt kinases, amplification of Akt, and overexpression or amplification of eIF4E or S6K1.(3,9) The mTOR signaling pathway is also up-regulated in various carcinoma cell lines and in human ovarian and breast carcinomas.(10)
Therefore, targeting mTOR kinase may lead to an antitumor effect in several types of cancers via cell cycle arrest and cell growth inhibition. There are several mTOR inhibitors available today, including rapamycin (sirolimus) and its analogs CCI-779 (temsirolimus), AP23573, and RAD001 (everolimus). Recently, RAD001 (everolimus) showed promising antitumor activity against low-to-intermediate grade neuroendocrine tumors and renal cell carcinomas.(11,12) Moreover, several phase II studies in breast cancer were performed to evaluate the safety and efficacy of temsirolimus or everolimus as a component of a combined multi-drug regimen or as a single drug, and showed benefit from the combined regimen.(13) However, a large phase III study of letrozole alone or in combination of temsirolimus in postmenopausal women with breast cancer failed to demonstrate any benefit from the combination.(14) It is possible that this failure is not due to the lack of efficacy of this combination, but to treatment of patients who are not specifically selected for mTOR pathway activation. Indeed, there is no predictive marker that identifies PI3K/Akt/mTOR pathway-dependent tumors.
Expression of Akt and mTOR in breast cancer has been studied, but various rates of expression have been reported, with conflicting findings regarding their prognostic influence and association with ER or erbB-2 status. Here, we (1) evaluated expression levels of activated Akt (phosphorylated Akt, p-Akt) and mTOR (phosphorylated mTOR, p-mTOR) in breast cancer patients, and (2) analyzed the relationship between their expression and clinicopathological features of breast cancer such as tumor size, lymph node status, stage of disease, hormone receptor and erbB-2 status. Their prognostic impact on a large population of patients with breast cancer was also assessed in order to see if the data would support the strategy of targeted therapy of breast cancer using mTOR inhibitors.
METHODS
Tissue samples and clinicopathologic data
Sequential archival samples from patients who had undergone surgical treatment and were diagnosed as having primary breast carcinoma at Korea University Guro Hospital between April 1992 and October 2006 were involved in the study. Cases with distant metastases at the time of diagnosis were excluded and 730 cases were initially included in this study. Of the initial 730 cases, 105 had to be excluded due to staining failure resulting from section folding or absence of tumor cells. Of the remaining 625 cases, 65 were excluded due to insufficient clinical data. Finally, a total of 530 invasive carcinomas and 30 ductal carcinomas in situ (DCISs) were evaluated in our study. For all patients, detailed clinicopathologic data including patient age, lymph node status, tumor size, tumor grade, and survival data were obtained from hospital records. Grading of carcinomas was performed according to the Nottingham combined histologic grading system using the method of Elston and Ellis.(15) The median follow-up time was 58.5 months.
Tissue microarray construction
For tissue microarray (TMA) construction, hematoxyline and eosin stained sections of each tumor were examined. Representative areas of tumors were selected and marked on the corresponding paraffin block. The selected area in the corresponding paraffin block was punched out and embedded in microarray blocks. One or two 2 mm cores of the selected area in the corresponding paraffin block from each case were arrayed.
Immunohistochemistry
For immunohistochemical analysis, serial 4 µm sections of the TMA block were mounted on electrostatic slides, heat-dried at 56℃ for 30 min, deparaffinized in xylene, and rehydrated through graded concentrations of ethanol. Antibody and antigen retrieval methods are summarized in Table 1. Slides were incubated in a solution of 3% hydrogen peroxidase in methanol for 15 min to block endogenous peroxidase activity. Slides were incubated in 0.3% bovine serum albumin/1X Tris-buffered saline (TBS) for 20 min to reduce nonspecific background staining. A primary antibody was applied for 30 min at room temperature. After a series of TBS rinses, bound antibody was detected using a polymer secondary antibody from the DAKO EnVision+ system (DAKO, Carpinteria, USA). The slides were rinsed with a TBS series and visualized after a 10 min incubation of liquid 3, 3'-diaminobenzidine in buffered substrate (DAKO, Carpinteria, USA) for 10 min. The slides were counterstained with hematoxylin.
Assessment of immunohistochemical staining
We assessed immunohistochemical staining of TMA sections in a semiquantitative manner. Expression levels of p-Akt and p-mTOR were categorized into three groups based on both intensity and proportion of cancer cells with cytoplasmic or nuclear staining. This was done according to a previously described scoring system with a slight modification.(9) Tumors without a reaction were scored as 0 (negative); tumors with 1-50% of cells showing weak staining or 1-10% of cells with strong staining were scored as 1; tumors with >50% of cells with weak staining or >10% of cells with strong staining were scored as 2.
In regard to ER and progesterone receptors (PR), cancer cells with nuclear staining were considered as immunoreactive ones, and evaluated for labeling index and staining score. ER and PR scoring was done using the Allred scoring method.(16) Briefly, a proportion score was assigned that represented the estimated proportion of positive tumor cells on each core as follows: 0, none; 1, <1/100; 2, 1/100-1/10; 3, 1/10-1/3; 4, 1/3-2/3; 5, >2/3. An intensity score was assigned that estimated the average staining intensity of positive tumor cells in each core as follows: negative, 0; weak, 1; intermediate, 2; and strong, 3. The proportion score and the intensity score were added to obtain a total score. Cases with a total score of 3 or more were considered positive.
With regard to erbB-2, a cancer cell with membranous staining was considered as an immunoreactive one, and was evaluated to determine a score. Membranous staining of erbB-2 was evaluated using the HercepTest® (DAKO, Carpinteria, USA) scoring method as follows: cores with more than 10% of strong membranous staining, 3; cores with more than 10% of moderate staining, 2; cores with more than 10% of weak staining, 1. erbB-2-positive cases were defined as those for which the score was 3.
Fluorescence in situ hybridization
ErbB-2 gene amplification was determined using the Path Vysion® (Vysis, Downers Grove, USA) HER2 DNA Kit containing 2 DNA probes that are directly labeled with a spectrum orange fluorophore (HER2 gene locus on band 17q11.2-12). A spectrum green fluorophore-labeled chromosome 17 enumeration probe (CEP17; band 17p11.1-11.1) was used following the manufacturer's instructions. According to the recent guidelines of the American Society of Clinical Oncology and the College of American Pathologists (ASCO/CAP),(17) a sample with an HER2/CEP17 ratio greater than 2.2 was considered amplified.
Western blot
To validate the specificity of the antibodies used in this study, western blot analysis was performed in the cell line and in lysates of freshly frozen tissue from 5 breast tumors. Freshly frozen tissues were cut into sections and lysed in NP-40 lysis buffer (50 mMol/L of Tris hydrochloride, pH 7.4; 150 mMol/L of sodium chloride; 0.5% NP-40 (Aldrich, St Louis, USA); 50 mMol/L of sodium fluoride; 1 mMol/L of sodium orthovanadate; 1 mMol/L of phenylmethylsulfonyl fluoride; 25 µg/mL of leupeptin; and 25 µg/mL of aprotinin). The supernatants were cleared by centrifugation. Protein concentrations were measured using a Coomassi plus protein assay reagent (Pierce Chemical, Rockford, USA).
For western blot analyses, 40 µg of crude extracts were boiled in sodium dodecyl sulfate sample buffer; the proteins were resolved by sodium dodecyl sulfate-polyacrylamide gel electrophoresis, transferred to a nitrocellulose membrane (Bio-Rad Laboratories, Hercules, USA), and probed with the primary antibody for erbB-3 (MS-313-P1; NeoMarkers, Fremont, USA). After the blots were incubated for another hour at room temperature with a horseradish peroxidase-labeled secondary antibody (goat antimouse IgG; Perkin Elmer, Boston, USA), signals were detected using the Enhanced Chemiluminescence assay (Amersham Life Science, Arlington Heights, USA) per the manufacturer's instructions. Positive control samples were included in MCF-7, SK-Br3, and MDA-MB-468 cell lines.
Statistical analysis
Correlations between 1) expression levels of p-Akt or p-mTOR, and 2) clinicopathologic parameters were assessed with 2×3 or 3×3 tables using a Fisher's exact test because these variables were measured as qualitative (ordinal or categorical) data. The influence of levels of p-Akt or p-mTOR on disease-free survival (DFS) was estimated using the Kaplan-Meier method. Survival was calculated from the time of the initial diagnosis to the date of last contact (or the date of death if the patient was deceased). DFS was defined as the interval (measured in months) from the date of initial diagnosis to the date of the first local recurrence or distant metastasis. The association between intervals and levels of p-Akt or p-mTOR was tested using the log-rank test. To determine the effect of levels of p-Akt or p-mTOR on cancer-specific survival, multivariate analysis was performed using the Cox proportional hazard survival regression method, controlling for age, tumor size, tumor grade, status of lymph node metastasis, expression of ER, and PR. p-values of less than 0.05 were considered statistically significant. Statistical analysis was performed using the SPSS Statistical Package (version 12.0.1; SPSS, Chicago, USA).
RESULTS
Clinicopathologic characteristics
Of the 530 invasive carcinomas, most cases were ductal (497 cases, 93.8%). The distribution of 530 invasive carcinoma cases according to clinicopathologic characteristics at diagnosis is summarized in Table 2. The median age at the time of diagnosis was 46.0 yr (range, 26-85 yr). A total of 120 cases (22.6%) were grade 1, 247 cases (46.4%) grade 2, and 141 cases (26.6%) grade 3. Information on tumor size and lymph node status was available for 515 cases. Tumor size ranged from 2 mm to 10 cm in maximal diameter. A total of 234 cases (44.2%) had tumors 2 cm or less in its greatest dimension (T1), 259 cases (48.9%) had tumors between 2 and 5 cm (T2), and 22 cases (4.2%) with tumors more than 5 cm (T3). A total of 227 cases (42.9%) showed lymph node metastasis.
ErbB-2 status was evaluated with immunohistochemical staining or FISH on 502 carcinomas. Among these cases, 120 (23.9%) showed positivity on immunohistochemical staining or gene amplification on the FISH test. ER status was available on 526 carcinomas. ER expression was seen in 299 cases (56.4%).
Frequency of p-Akt and p-mTOR expression
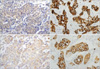
Using the criteria described above, weak and strong p-Akt staining were detected in, respectively, 6 and 21 of 30 (20.0% and 70.0%) DCISs (Figure 1A, B). In 530 invasive carcinomas, there were 180 (34.0%) samples with weak p-Akt expression and 288 (54.3%) with strong p-Akt expression (Figure 2A, B). Of the 30 DCISs, 7 cases (23.3%) showed weak p-mTOR expression and 21 (70.0%) cases exhibited strong expression (Figure 1C, D). In invasive carcinomas, weak and strong p-mTOR expression was observed in 136 (25.7%) and 207 (39.1%) of 530 cases (Figure 2C, D). There were differences in expression of p-mTOR between DCISs and invasive carcinomas (p=0.001). A significant correlation was seen between p-Akt and p-mTOR expression in invasive carcinomas (p=0.002) in Fisher's exact test. Consistent with immunohistochemical findings for p-mTOR, the results of western blot analysis were in accord with those of immunohistochemical analysis in the 5 breast tumors (Figure 3).
Association with p-Akt and p-mTOR expression and clinicopathological parameters
Tables 3, 4 show the relationships between expression of p-Akt or p-mTOR and clinicopathologic parameters of invasive carcinomas. Expression of p-Akt was associated with expression of ER (p=0.045) and PR (p=0.003), and was inversely associated with metastasis of lymph nodes (p<0.001). However, no association was noted with erbB-2 status (p=0.167), tumor grade (p=0.884), and tumor size (0.306). Expression of p-mTOR was associated with expression of ER (p=0.040) and PR (p=0.009), and was inversely associated with tumor size (p<0.001). Expression of p-Akt and p-mTOR each showed a significant association with early stage (p=0.027 and p=0.002, respectively).
Patient survival according to expression of p-Akt and p-mTOR
Of 530 patients with invasive carcinoma, 118 had local recurrence or distant metastasis, and 65 died of their disease. Concerning p-Akt and p-mTOR, patients with negative (score 0) or weak (score 1) expression were compared with those with strong (score 2) expression, because there was no difference between groups with score 0 and score 1 in the survival analysis. Univariate analysis using the Kaplan-Meier method together with the log-rank test was performed to investigate possible associations of DFS with p-Akt, p-mTOR and other clinicohistologic characteristics (Table 5). Strong expression of p-Akt, positivity for ER and PR, and low tumor grade were associated with longer DFS. The 5-yr DFS rate was 70.5% in tumors with negative or weak expression of p-Akt, whereas it was 79.9% in p-Akt strong-positive tumors (p=0.004). This difference is shown in Figure 4. Patients with large tumor size, metastasis in the lymph nodes and young age had decreased DFS. In contrast to p-Akt, p-mTOR expression showed no statistical significance in DFS (p=0.136) (Figure 5).
As shown in Table 6, multivariate regression analysis using the Cox proportional hazards regression model, including p-Akt, p-mTOR, ER, PR, tumor grade, tumor size, status of lymph node metastasis and age, demonstrated the tumor size (hazard ratio, 1.730; p=0.009) and the status of lymph node metastasis (hazard ratio, 2.247; p<0.001) to be independent prognostic factors for DFS. None of the other parameters that were studied showed a significant effect on DFS, although strong expression of p-Akt tended to be associated with longer DFS (p=0.066).
DISCUSSION
The present study evaluated the expression of p-Akt and p-mTOR. We found a correlation between p-Akt and p-mTOR, indicating that Akt is a main up-regulator of the downstream target, mTOR, although there are complex regulatory pathways upstream of mTOR. p-Akt exhibited a high incidence of weak and strong expression, 34.0% and 54.3% respectively, in invasive breast carcinomas. Frequency of weak and strong expression of p-mTOR was 25.7% and 39.1% in the same samples. So far, expression of activated Akt and/or mTOR has been evaluated by immunohistochemistry in various human cancers including carcinomas of breast, stomach, lung, ovary and liver, and brain glioblastoma.(9,18-24) In breast carcinoma, the rate of p-Akt and p-mTOR overexpression has been reported as 38% to 93.5% and 24% to 69.7%, respectively. This broad range of reported frequencies of both proteins may be due to various factors such as the different criteria for positivity, detection techniques, and patient sample size.
The results of this study showed that TOR is more frequently activated in DCISs than in invasive breast carcinomas (p=0.001). These data are in agreement with recent studies. Bose et al.(20) found high levels of p-Akt and p-mTOR in DCISs as well as in invasive ductal carcinomas, and p-mTOR was more frequently found in DCIS than in invasive ductal carcinomas. Zhou et al.(9) reported similar data regarding expression of p-Akt and p-mTOR. In a study with hepatocellular carcinoma and adenoma, phosphorylated mTOR was detected in 15% of hepatocellular carcinomas and 33% of hepatic adenomas, immunohistologically.(24) Taking these results into account, it is postulated that activation of the PI3K/Akt/mTOR pathway might be an early event in mammary carcinogenesis.(9)
In the analysis of clinicopathologic parameters, we observed a positive correlation of p-Akt or p-mTOR with ER and PR, but not with erbB-2. The direct and indirect activation of the Akt/mTOR pathway by erbB-2 in breast carcinomas was suggested in many studies.(9,25) Although down-stream regulation of the PI3K/Akt/mTOR pathway by the receptor tyrosine kinase family was demonstrated in some studies,(18,26) others failed to show such a correlation.(20,21) Instead, other reports suggested ER as an upstream regulator of the Akt/mTOR pathway.(19,22) In a study of 692 invasive breast carcinomas, Panigrahi et al.(19) found a positive significant correlation of p-AKT with ER, as was found in our study which suggests the ER as a potential upstream component in development of breast carcinoma rather than PTEN or erbB-2.
Our results suggest the usefulness of mTOR as a therapeutic target of breast cancer as well as revealing the pathogenesis of breast cancer. In a recent phase II clinical study, responses to everolimus occurred only in patients with ER-positive breast cancer.(27) The Akt/mTOR pathway stimulated by ER can be considered as an underlying mechanism for the results of that clinical trial.
We investigated the prognostic significance of these activated proteins using Kaplan-Meier survival analysis. In univariate analysis, strong expression of p-Akt had a favorable effect on DFS. This effect was not found on multivariate analysis with p-Akt, p-mTOR, tumor grade, tumor size, status of lymph node metastasis, status of ER, PR and age. These findings suggest tumor size and lymph node metastasis as independent prognostic factors for decreased DFS. Although the prognostic value of p-Akt in our study is not clear, some previous studies have observed a correlation between higher p-Akt expression and poorer clinical outcomes in breast carcinomas,(9,18,26) whereas other reports have not demonstrated any correlation between p-Akt or mTOR expression and clinical outcomes.(21)
There are several studies in agreement with our findings. A study by Panigrahi et al.(19) reported that p-Akt expression correlated inversely with adverse tumor variables such as higher grade, larger invasive tumor size, and the Nottingham prognostic index, but Kaplan-Meier survival analysis and multivariate analysis did not show an association with p-Akt immunopositivity and survival. In a study with 63 patients with endometrioid-type endometrial carcinoma, Mori et al.(28) obtained similar results-that higher p-Akt expression appeared to be associated with longer relapse-free survival in univariate analysis. Of note is that these results, including ours, are not compatible with the theory that Akt promotes tumor growth and aggressiveness by an anti-apoptotic function and pro-cell cycle entry properties. To explain this discordance, Mori et al. suggested that higher p-Akt expression correlates with better prognoses for tumors in estrogen-responsive tissues, including breast, ovarian, and endometrial cancer tissue.
Likewise, Al-Bazz et al.(22), in a recent study with 49 invasive breast carcinomas using immunoblot analysis, found a significant relationship between p-Akt levels and ER status. These authors also observed that intermediate levels of p-Akt were associated with a lower probability of recurrence in univariate analysis, while none of the p-Akt levels showed statistical significance in multivariate analysis. In contrast, the studies, which showed correlated expression of Akt and erbB-2, revealed a significant association between p-Akt and poor prognosis.(9,26) Taking these results into account, the relatively favorable effect of p-Akt on survival in our study may be derived from the well-established relationship between ER positivity and good prognosis, or the loss of ER positivity in the late stage of breast carcinomas. In addition, possible cross-talk between the ER pathway and the PI3K/Akt/mTOR pathway controlled by tyrosine kinase receptor family members might be considered as an underlying mechanism for this survival result.
In comparison with p-Akt, p-mTOR has been less often studied in breast tumors.(9,20) mTOR seems to be less highlighted than other molecules involved in the PI3k/Akt/mTOR signaling pathway such as PTEN, PI3K, S6K1 or Akt do. Preclinical studies suggested that mTOR or p-mTOR is not useful as a predictive marker for rapamycin or its analogues in breast cancer cell lines, and demonstrated that patients with p-mTOR expression show a significantly lower DFS rate and that p-mTOR does not show a significant association with ER.(21,29) In our study, p-mTOR expression is not associated with DFS but correlates with ER expression. These findings suggest that the effect of p-mTOR on survival might also be influenced by the association of p-mTOR with ER status.
Although many clinical trials are going on to evaluate the effect of mTOR inhibitors in the treatment of various tumors, who will derive a benefit from mTOR inhibition remains unclear. Thus, there is the need to identify predictive markers to select suitable patients for mTOR inhibition. Therefore, several components of the PI3K/Akt/mTOR signaling pathway are under intensive investigation as predictors for mTOR inhibition as well as potential therapeutic targets. In a clinical trial in patients with advanced renal cell carcinoma, p-Akt was suggested as a predictive marker for treatment with rapamycin and its analogues.(30) An understanding of the expression and functions of various components of the PI3K/Akt/mTOR pathway would be important to the application of mTOR in the treatment of cancer in this era of individually tailored medicine.
CONCLUSION
PI3K/Akt/mTOR pathway is active in DCIS as well as in invasive carcinoma of breast. The PI3K/Akt/mTOR pathway can be influenced by ER more than by erbB-2, and the prognosis in breast carcinoma may depend on the relationship between the Akt/mTOR pathway and ER status. Our data will contribute to the development and application of the PI3K/Akt/mTOR signaling pathway in targeted therapy.










 XML Download
XML Download