

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the most dreadful cancer for the women in the United States, and has become the most prevalent cancer in women even in the Asian countries.(1) Before the introduction of the concept of the breast conservation, more radical operations such as radical or modified radical mastectomy had been used for the most of the breast cancer patients. After the incorporation of the breast-conserving operation into the armamentarium of the therapeutic modalities against the breast cancer after becoming to get the widespread approval as a standard cancer treatment, the need of the external radiation therapy for the breast remained after the lumpectomy has been increasing.(2) In addition, many of the metastatic foci from the index tumor should be considered as the therapeutic targets for the radiation.(3) Though ionizing radiation treatment is one of the strong modalities can be used, there should always be the hazard of harming adjacent normal tissues around the tumor. Hence, many studies have been done to enhance the radiation effects in the various cancer cells or sensitize the tumor cells before radiation.
Inducible cyclooxygenase, cyclooxygenase-2 (COX-2), that is integrated in the prostaglandin E2 (PGE2) synthesis, has been shown to be an important mediator of tumorigenesis in many malignancies.(4,5) Celecoxib, one of the selective COX-2 inhibitors, has shown its efficacy in the prevention and even treatment of breast cancer, by inhibiting COX-2 activities on the human breast cancer cells.(6) When in combination with ionizing radiation, celecoxib showed better treatment response to reduce tumor growth.(7) Recently, the melanoma differentiation-associated gene 7 (mda-7) has been shown to enhance the effectiveness of radiation therapy in lung cancer cells in vitro and in vivo.(8) We sought to evaluate whether the combination of celecoxib and adenoviral mediated delivery of mda-7 (Ad-mda7) could enhance radiosensitization of human breast cancer cells in vitro.
METHODS
Cell lines
The estrogen receptor negative and HER2/neu negative MDA-MB-436 and MDA-MB-468 human breast cancer cells were obtained from the American Type Culture Collection (ATCC, Manassas, USA). The cells were maintained in high glucose Dulbecco's modified Eagle medium/F-12 media supplemented with 10% fetal bovine serum with 10 mmol/L L-glutamine, 100 U/mL penicillin, and 100 µg/mL streptomycin (GIBCO Invitrogen Co., Grand Island, USA) in a humidified 37℃, 5% CO2 atmosphere.(6)
Adenovirus transduction and celecoxib treatment
As described previously,(6) the recombinant adenovirus vectors carrying the mda-7 gene and the luciferase reporter gene (Ad-luc) were obtained from Introgen Therapeutics (Houston, USA). One times 106 cells in 100-mm culture plates were transduced with Ad-mda7 or Ad-luc at a multiplicity of infection of 1,000 or 2,000 viral particles (vp) per cell (50 or 100 plaque-forming units/cell) for MDA-MB-436 and MDA-MB-468 cell lines, respectively. Celecoxib was dissolved in dimethyl sulfoxide and added to cell culture media at a final concentration less than 0.1% (to not affect cell survival) and then introduced into the cultures at a dose of 50 or 30 µmol/L for MDA-MB-436 and MDA-MB-468 cells, respectively. The doses of vector and celecoxib were selected to ensure toxicity of less than 50% to compare the combinatorial effect of Ad-mda7 and celecoxib.
Clonogenic cell survival assay (CSA)
Clonogenic survival assay was applied to determine whether celecoxib and Ad-mda7 or both enhance radiosensitivity of the MDA-MB-436 and MDA-MB-468 human breast cancer cells in vitro. Cells in culture were treated with celecoxib, Ad-mda7 or both for 3 days, which were then to be irradiated with different level of doses (0, 2, 4 ,6 Gy) of γ-rays using a 137Cs source (3.7 Gy/min). The cells were assayed for colony-forming ability by plating them again in predetermined certain cellular numbers into 100-mm dishes in the unconditioned media afterwards. On completion of 14 day incubation, the cells were stained with 0.5% crystal violet in absolute ethanol to make all the colonies to be seen clearly, and colonies with more than 50 cells predetermined under the light microscope were counted manually. Survival curves after the radiation following each treatment including control were outlined after calibrating for the toxicity produced by celecoxib, Ad-mda7, or both. Clonogenic survival curves were generated from three independent experiments by taking the average survival levels using least-squares regression by the linear-quadratic model.(9)
Fluorescence activated cell sorting (FACS) and cell cycle analysis
All the cultures were subconfluent at the time of harvest. Harvested cells were fixed with ice-cold 80% ethanol, stained with propodium iodide (PI) (Sigma, St. Louis, USA), and analyzed with a flow cytometer (EPICS XL-MCL; Coulter, Miami, USA) as described previously. Cells floating in the medium and trypsinized adherent cells were washed and pelleted. The collected cells were washed and then stained with Annexin V-fluorescein isothiocyanate (FITC) PI by using an Annexin V/FITC apoptosis detection kit (BD Biosciences, Franklin Lake, USA). The 5-bromo-2-deoxyuridine/terminal deoxynucleotidyl transferase (TdT)-mediated 2'-deoxyuridine 5'-triphosphate (dUTP)-biotin nick end labeling assay (TUNEL) (APO-Direct; BD Biosciences) was performed according to the manufacturer's protocol. Briefly, paraformaldehyde-fixed cells were washed and incubated with staining solution (10 µL of TdT reaction buffer, 0.75 µL of TdT enzyme, and 8 µL of FTC-dUTP) overnight. The following day, cells were rinsed and resuspended in 1 mL of PI/RNase solution. After incubation in the dark for 30 min at room temperature, flow cytometry was performed to obtain the percentage of apoptotic cells. Cell cycle was analyzed with a program combined with the flow cytometry (Multicycle; Phoenix Flow System, San Diego, USA). The TUNEL assay to identify the DNA fragmentation (APO-BRDU kit; Pharmingen, San Diego, USA) was performed according to the manufacturer's instructions. Briefly, the cells (2×106) were fixed in 1% paraformaldehyde and washed in phosphate-buffered saline (PBS). They were then suspended in 70% ethanol and stored at -20℃ until use. The cells were resuspended in a staining solution containing TdT and Br-dUTP and incubated overnight at room temperature in the dark. Then the cells were rinsed and resuspended in a fluorescein-labeled anti-BrdU antibody solution, followed by exposure to a propidium iodide/RNase A solution (0.5 mL), and analyzed by flow cytometry.(6)
PGE2 measurements
To determine the concentration of PGE2, cells were seeded at a density of 1×106 cells/100-mm plates and treated with celecoxib, Ad-mda7, or a combination of both agents. After 72-hr incubation, 3 µL of arachidonic acid (1 mmol/L) was added to the culture medium to boost the PGE2 production for 30 min. The supernatant was collected and stored at -80℃ until PGE2 concentration was measured by using an enzyme-linked immunoassay kit (Cayman Chemical, Ann Arbor, USA) according to the manufacturer's manual. The final results from the triplicated values were expressed as pg.(6)
Immunoblotting
Cells were lysed and protein concentration was determined by using the BioRad Assay (Bio-Rad Laboratories, Hercules, USA). Lysates were analyzed by Western blot analysis by using 10% sodium dodecylsulfate gels. Lanes were loaded with 50 µg of protein and electrophoresed for 2 hr at 90 V. Gels were transferred to nitrocellulose membranes that were blocked with 5% nonfat dry milk and incubated with primary antibodies of COX-2 (Cayman Chemical Co., Ann Arbor, USA), β-catenin (Santa Cruz Biotechnology Inc., Santa Cruz, USA), Akt (Cell Signaling, Beverly, USA), and p-Akt (Cell Signaling) overnight at 4℃. Membranes were washed and incubated with secondary antibody for 1 hr at room temperature. Membranes were then developed, and protein signals were detected by using enhanced chemiluminescence Western blotting detection reagents (Amersham Biosciences, Buckinghamshire, UK). Membranes were incubated with an antibody against β-actin (Santa Cruz Biotechnology Inc.) to assess equal protein loading, and results were subjected to densitometry.(6)
Statistical analysis
Statistical analysis was performed between control and treated groups and among the different experimental groups. Comparisons of means were carried out by using the paired t-test. The densitometry of the Western blots was also analyzed for significance by the paired t-test. Differences with a value of p<0.05 were considered to be statistically significant. The significance of the results was determined by the paired t-test.
RESULTS
Enhanced expression of MDA7 protein after the combination of celecoxib and Ad-mda7
Unexpectedly, we got the increased MDA7 protein expression, confirmed by immunoblotting, after treating cells with celecoxib and Ad-mda7, compared to the either alone treatment (Figure 1).
Increased efficacy of radiosensitization after celecoxib, Ad-mda7, or both
After three-day preconditioning of these two cell lines with celecoxib, Ad-mda7 or both to determine the possible effect of radiosensitization onto the cells in vitro, we got the radiation dose-dependent survival reduction in two cell lines tested (Figure 2). Treatment of celecoxib and Ad-mda7 alone shifted the survival curve to the left, compared to the control in a certain dose of radiation. But the combination of the celecoxib and Ad-mda7 made that shift far to the left. The grade of deduction of the cell survival after CSA could be expressed by enhancement factor (EF): At 0.1 cell survival level, EF of celecoxib was 1.35, Ad-mda7 was 1.37, and the combination was 1.75 in MDA-MB-436, and celecoxib 1.12, Ad-mda7 1.20, and the combination 1.44 in MDA-MB-468.
At a radiation dose of around 2 Gy, shoulder formation easily seen in control could be eliminated after the combination pretreatment in advance to the radiation in both cell lines.
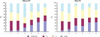
Flow cytometry and apoptosis
In MDA-MB-436 cells, we already proved that the combination treatment with celecoxib and Ad-mda7 was superior to the either alone treatment without additional radiation treatment (p=0.02 for celecoxib and p=0.08 for Ad-mda7) (Figure 3).(6) The apoptosis seemed to be increased more, after the combination treatment followed by radiation exposure, compare with celecoxib (p=0.05) or Ad-mda7 (p=0.08). In MDA-MB-468 cells (Figure 4), the apoptosis seemed to be more robust in Ad-mda7 than celecoxib treatment before radiation (p=0.01). There was no significant difference between Ad-mda7 and the combination. After the radiation, the combination resulted in the most significant increase in the apoptosis compared with any other monotherapy (p=0.001 for celecoxib, p=0.03 for Ad-mda7). And the Ad-mda7 had much influence on the apoptosis than celecoxib (p=0.001).
Effect on the cell cycle arrest
Previous studies with tumor cell lines have documented that Ad-mda7 induces G2/M phase arrest, whereas celecoxib induces a G1 block. The combination treatment in MDA-MB-436 cells before radiation exposure resulted in an increase in cells in S-phase compared with celecoxib or Ad-mda7. Celecoxib blocked more cells at the G1 checkpoint than Ad-mda7, whereas Ad-mda7 monotherapy resulted in a G2/M block. After the radiation, Ad-mda7 and the combination resulted in the increased population in S-phase fraction (p=0.04 and p=0.01, respectively) than celecoxib monotherapy, whereas celecoxib blocked more cells at the G1 checkpoint. The percentage of G2/M phase fraction in the combination group was far less than the celecoxib monotherapy (p=0.02), and a little bit less than the Ad-mda7 treatment. In MDA-MB-468 cells before the exposure to the radiation, celecoxib holds more cells in G1 phase than Ad-mda7 or the combination treatment (p=0.08 and p=0.047, respectively). The addition of celecoxib to Ad-mda7 resulted in the decrease of S phase fraction (p=0.03). Moreover, the combination treatment significantly accumulated cells in G2/M phase, compared with Ad-mda7 monotherapy (p=0.04). After the radiation treatment, celecoxib monotherapy resulted in the increased S phase fraction compared to the Ad-mda7 treatment (p=0.02).
PGE2 levels in the culture media after the combination of celecoxib and Ad-mda7
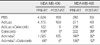
We already showed that the combination treatment of Ad-mda7 and celecoxib could reduce the biosynthesis of PGE2 in the human breast cancer cells in vitro.(6) We thought that we could see the similar results on the inhibition of PGE2 synthesis by synergistic inhibition of Ad-mda7 and celecoxib. In MDA-MB-436 cells, we could get the same results of our previous report before irradiation. The combination and celecoxib monotherapy showed significant inhibition of PGE2 production compared with the controls (p<0.05). On completion of radiation following preconditioning, the inhibition of PGE2 synthesis was more profound in celecoxib monotherapy (p=0.004) and the combination treatment (p=0.004). But, we failed to get the statistically significant decrease of PGE2 synthesis after Ad-mda7 monotherapy. In MDA-MB-468 cells, slightly different from the results of MDA-MB-436 cells, we could get the significant changes of PGE2 production after either monotherapy of Ad-mda7 and celecoxib along with the combination of Ad-mda7 and celecoxib. Before radiation exposure, celecoxib and Ad-mda7 monotherapy effectively reduced the production (p=0.016 and p=0.005, respectively), and the combination decreased the synthesis far greater than monotherapy (p=0.004). After the radiation exposure, this cell line showed significant reduction of the amount of PGE2 in Ad-mda7 and the combination (p=0.032 and p=0.011, respectively). Unexpectedly, celecoxib monotherapy failed to reduce the PGE2 biosynthesis effectively after the radiation (p=0.064). Due to the fact that we couldn't get the expression of COX-2 in the MDA-MB-468 cells after the radiation exposure even in the control group, we thought that radiation may markedly interfere the action of COX-2 through the unknown mechanism (Table 1).
Ad-mda7 and celecoxib combination decreases expression of COX-2, Akt, and p-Akt
Ad-mda7 treatment is known to regulate negatively the expression of Akt and p-Akt.(10) Similar effects have been observed for β-catenin expression after Ad-mda7 transduction in lung and breast carcinoma cell lines.(10) To elucidate the role of Ad-mda7 and celecoxib on the expression of representative prosurvival markers after the combination of Ad-mda7 and celecoxib, Western blots were preformed to analyze steady-state levels of COX-2, Akt, p-Akt, and β-catenin (Figure 5). In MDA-MB-436 cells, Akt, p-Akt, and COX-2 expression levels were decreased after cotreatment without radiation exposure (p<0.05). The expression of Akt is somewhat repressed by celecoxib compared with control (p=0.05). Ad-mda7 increased p-Akt levels, although the increase was also observed with Ad-luc, suggesting that the effect was not MDA-7 protein-dependent. The combination of Ad-mda7 and celecoxib reduced p-Akt expression by >70% compared with control and by approximately 50% compared with celecoxib monotherapy. Both Ad-mda7 and celecoxib reduced COX-2 expression, and further COX-2 inhibition was seen by the combination treatment in MDA-MB-436 cells. After the radiation exposure, MDA-MB-436 cells showed much decrease in Akt expression more than 60% and about a half compared with either monotherapy, even though we failed to get the significant differences in the densitometry. The level of expression of p-Akt was markedly repressed in the combination treatment (p=0.01), while each monotherapy resulted in increase of p-Akt expression. Though the β-catenin expression was reduced in the combination treatment, it was not significant. COX-2 level of expression showed significant decrease in the combination treatment compared with celecoxib (p=0.02) or Ad-mda7 (p=0.049). In MDA-MB-468 cells before the radiation exposure, the expression of Akt was less than a half of the control, and approximately 60% of celecoxib treatment. The combination seemed to induce the regression of Akt expression. Ad-mda7 effectively reduce the phosphorylation of Akt (p=0.001), while we could see the decrease in that expression in combination treatment but failed to get the significance. β-catenin expression was irrelevant to the preradiation treatment. COX-2 expression was significantly reduced after Ad-mda7 transduction (p=0.01). After the radiation treatment in the MDA-MB-468 cells, we failed to get the differences in the expression of Akt, and p-Akt, even though there was some of decrement in expression of that protein. Ad-mda7 brought significant changes in the level of β-catenin in Ad-mda7 transduction followed by the radiation. There was none of the COX-2 expression in this cell line.
DISCUSSION
Recent progresses in the diagnosis and treatment of the breast cancer have made us to experience many improvements in the patients'care and treatment results. Most of all, increasing use of breast-conserving surgery and radiotherapy for the early breast cancer patients is one of the most striking and patient-forward changes ever made without compromising oncologic principles and therapeutic results.(2,11) Before the introduction of this idea of the breast conservation, more radical operations such as radical or modified radical mastectomy had been used for the most breast cancer patients, while giving them many of the mutilated body images as a woman. Though ionizing radiation treatment following breast-conserving operation or not is one of the strong modalities can be used, there should always be the hazard of harming adjacent normal tissues around the tumor or the radiation field. Therefore, there have been many demands how to enhance the radiation effects in the various cancer cells or sensitize the tumor cells before radiation in order to decrease unwanted adverse reactions while getting desirable therapeutic effects with less radiation doses.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are well known for its effect of enhancing radiosensitivity of tumor cells while protecting irradiated immune cells.(12) NSAIDs nonselectively inhibit the production of prostaglandins (PGs) from arachidonic acid by inhibiting the activity of cyclooxygenase-1 (COX-1) and COX-2. While COX-1 is expressed ubiquitously in many tissues, COX-2 can be induced by various stimuli including several oncogenes. Recent report implicating possible interrelation between elevated COX-2 expression and reduced patient survival after radiation,(13) leads to the finding of protective role of COX-2 by making prostaglandins as tumor survival factors after irradiation. Even though nonselective inhibitors of both COX isoforms have shown increased radiosensitivity in vitro, these kinds of drugs should be used deliberately owing to their own toxicity including gastrointestinal trouble. Therefore, considerable interest has been focused on the selective COX-2 inhibitors, such as celecoxib, for the possible role as a radiosensitizer. Recently, in vivo data suggest the probable effect of selective COX-2 inhibitor to increase the response of tumor cells to radiation without increasing radiation injury to the normal surrounding tissues.(14) Synergy between celecoxib and irradiation was reported, even in tumors where COX-2 expression is confined to the tumor neovasculature, by inhibiting COX-2 derived PGE2.(7,15)
Recently, the melanoma differentiation-associated gene 7 has been shown to enhance the effectiveness of radiation therapy in lung cancer cells in vitro and in vivo.(8) We already showed synergistic effect by the combination of these two in vitro.(6) But, there have not been any study to elucidate possible role of the combination treatment with celecoxib and Ad-mda7 as a radiosensitizer in vitro, so we postulated that this combination may enhance the radiosensitivity of the human breast cancer cells. As expected, we could get the enhanced radiosensitization after treating MDA-MB-436 and -468 cells before irradiation with either celecoxib or Ad-mda7, but adding Ad-mda7 to celecoxib yielded the highest enhancement factor of all. The typical convex shape of shoulder formation (Figure 2) that can be seen at the lower radiation doses representing control group was almost totally eliminated after the combination treatment, which may suggest the possible and powerful radiosensitization effect of this combination.
Unfortunately, the underlying precise mechanism of the radiosensitizing activity of celecoxib has yet to be determined. Inhibitors of COX enzymes can cause cell cycle redistribution,(11) which could increase the cell killing effect of radiation if cells were positioned in the radiosensitive phases of the cell cycle (G2/M) at the time of radiation.(16) Celecoxib has shown its effect on the cell cycle arrest and to increase the fraction of G0/G1 and reduce S phase fraction in vitro.(17) In our result, the combination was far superior to either monotherapy and to the control on the induction of apoptosis in MDA-MB-436 cells, which could be translated as one of the main reasons how to increase the radiosensitivity in this cell line. A little different explanation can be deduced from the result of MDA-MB-468 cells. Before radiation exposure, there was no significant increase in the apoptosis after celecoxib monotherapy compared with Ad-mda7 treatment, but after the exposure, the cells showed marked increment of apoptosis in the combination group significantly. That meant the addition of celecoxib to the Ad-mda7 acted as a powerful radiosensitizer in MDA-MB-468 cells better than in MDA-MB-436 cells.
According to the previous studies, in addition to the induction of apoptosis, the cell cycle redistribution has an important meaning to the radiosensitization.(8,9) The effect of cell cycle redistribution of Ad-mda7 and celecoxib already documented. While we could see celecoxib blocks more cells at G1 checkpoint, Ad-mda7 treatment confined cells at radiosensitive G2/M phase. And the increased population at the S phase fraction could be seen after radiation exposure in MDA-MB-436 cells. In MDA-MB-468 cells, more cells were resided in the G1 phase after celecoxib monotherapy, and radioresistant S phase fraction could be decreased by the combination treatment, along with significant accumulation of cells into G2/M phase. We think this redistribution of cell cycles should be one of the mechanisms responsible for the radiosensitization after celecoxib and Ad-mda7 combination treatment. And the grade of radiosensitization may be dependent cell types and other unique characteristics of specific cells.
As previously documented, prostaglandins were the end product of cascade from the arachidonic acid, and COX-2 is one of the key enzymes to make PGs. And PGs is known to act against radiation to protect tumor cells to increase radioresistance.(18) So we explored the changes before and after the radiation after pretreatment with celecoxib and Ad-mda7. In MDA-MB-436 cells, aside from Ad-mda7 monotherapy, celecoxib and combination effectively inhibit PGE2 synthesis. However, Ad-mda7 showed significant inhibition of PGE2 in MDA-MB-468 cells along with celecoxib and combination treatment. According to the Western blots, there was no expression of COX-2 even in the control after radiation in MDA-MB-468 cells, and we think that might be the reason to inhibit PGE2 synthesis significantly even after Ad-mda7 in this cell line.
Among the complex network of cell signaling pathways initiated by ionizing radiation, receptor tyrosine kinases (RTKs) have been suspected to initiate cellular response to the radiation. After being phosphorylated by radiation exposure, many downstream transduction pathways after RTKs, including phosphatidylinositol 3'-kinase (PI3K) are initiated to enhance tumor cell proliferation and radio-resistance. Most of all the downstream targets of PI3K, serine-threonine protein kinase PKB/Akt (PKB or RAC) is one of the pivotal hubs in the regulation of downstream growth-promoting and cell prosurvival signals. Radiation seems to induce PKB/Akt activation in endothelial cells, which exerts to increase radioresistance both in vivo and in vitro.(19,20) Celecoxib inhibits cancer cell growth by inhibition of Akt phosphorylation.(6,21,22) And Ad-mda7 was documented to decrease the expression of Akt and p-Akt.(10)
Akt is activated by estrogen in estrogen receptor (ER) negative breast cancer cells in a ER independent manner.(23) As known previously, ER-negative breast cancer shows poorer prognosis and more recurrence or metastasis. Hence, this kind of breast cancer has more chance to have radiotherapy as adjuvant or salvage treatment, we tried to evaluate the change of expression of Akt and its phosphorylation. In addition to the various growth factors including epidermal growth factor, insulin-like growth factor-I, estradiol can affect the expression and activity of nuclear ER-α, by binding to membrane ER-α and interacting with ErbB2 to lead into tyrosine phosphorylation that results in the activation of phosphatidylinositol 3-kinase (PI3K) and Akt that may interact with nuclear ER-α.(24-26) So, even in ER-positive breast tumors, Akt pathway should be the one of the most important prosurvival route to escape therapeutic approaches. It was presented that celecoxib-induced apoptosis is mediated by Akt inactivation.(27) Inactivation of Akt following the inhibition of 3-phosphoinositide-dependent kinase-1 is the main proapoptotic pathway by which celecoxib exerts on the tumor cells.(28) We found that Akt, p-Akt, and COX-2 expression were significantly decreased, and the combination treatment decreased p-Akt expression by far in MDA-MB-436 cells. While the combination induced the regression of Akt expression in MDA-MB-468 cells, Ad-mda7 effectively and significantly reduce the p-Akt expression. Altogether with the findings of inducing MDA7 protein expression by adding celecoxib to Ad-mda7, we think the combination of celecoxib and Ad-mda7 can act against the phosphorylation of Akt to enhance radiosensitivity.
Ionizing radiation makes cell cycle stop after DNA damage, which usually occurs at G1/S and G2/M transitions, during which the damaged sites may be repaired.(29) And overexpressed β-catenin was known to attenuate this radiation-induced G1/S block.(30) That means β-catenin overexpression can accumulate the DNA damage following ionizing irradiation. However, we failed to get the statistically significant changes of β-catenin after any treatment. So we don't think have any role for boostering radiosensitivity by either Ad-mda7 or celecoxib.
Currently, we don't know the exact mechanism how to promote the expression of MDA7 protein by adding celecoxib into the culture media. But we think that this may be one of the reasons why we could get the better results of tumoricidal and radiosensitizing effect by combing these two treatments. This should be elucidated by further experiments. Though we tried to elucidate some possible mechanisms by which celecoxib and Ad-mda7 induce tumor radioresponse, many questions should be left behind for further investigation. Inhibition of COX-2 enzyme activity with or without Ad-mda7 has been proven to be effective to attenuate cancer growth and enhance therapeutic efficacy of chemotherapy and radiation. The present study or ours showed some possible explanation of radiosensitization. By combing Ad-mda7 and celecoxib, we could increase apoptosis, redistribute cell cycle into more radiosensitive G2/M phase, inhibit the synthesis of radioprotector PGE2, and inhibit prosurvival pathways of Akt and COX-2. However, more precise crosstalk between Ad-mda7 and celecoxib should be explored later. And the radiation itself may induce some radioprotective mechanisms even after treatment, many more studies should be followed to clarify whole network to selectively enhance radiosensitivity without triggering antiapoptotic network.
CONCLUSION
In conclusion, the expression of MDA-7 increased significantly by adding celecoxib, which shows the possible role of celecoxib boostering MDA-7. This combination may enhance their radiosensitizing effect through the inhibition of cellular repair after sublethal radiation damage and cell cycle redistribution. These possible mechanisms can be seen by CSA and cell cycle analysis. By the results of the cell cycle analysis and FACS, this effect may be interpreted as a product of the arrest of the cells at the radiosensitive G2/M phase of the cell cycle. This combination therapy right before the delivery of irradiation may be used to enhance the effectiveness of radiation therapy in breast cancer.




 XML Download
XML Download