

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
There is ongoing controversy regarding the management of papillary lesions that are diagnosed by core needle biopsy (CNB). The development of vacuum assisted biopsy now permits non-operative removal of papillary breast lesions. Our aim was to evaluate whether the papillary lesions diagnosed by vacuum assisted breast biopsy (VABB) can be followed up without further diagnostic excision.
Methods
From January 2003 to July 2009, a total of 4,655 US-guided mammotome excision were performed in 3,714 patients at Kangnam CHA Hospital. Out of 4,655 lesions, 156 lesions were proved to be papillary lesions. Among these, 82 lesions that had histologic findings that were consistent with benign papillary lesions and that were followed up for more than 2 years without further diagnostic surgical excision were collected and retrospectively analyzed. Ultrasonographic follow-up was done at 3-6 month intervals to assess for recurrence. The mean follow up period was 49.6 months.
Results
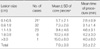
The pathologic diagnoses for the 82 lesions obtained via VABB were benign intraductal papilloma and papillomatosis. Half of the lesions were palpable and 50.0% (41 cases) were nonpalpable. Twenty eight lesions (34.1%) were classified as BIRADS category 3, 50 lesions (61.0%) were category 4A, 3 lesions (3.7%) were category 4B and only 1 lesion (1.2%) was category 5 according to the ultrasound exams. No local recurrence developed during the follow up period that needed surgical re-excision or rebiopsy. None of those diagnosed as benign lesions at VABB were upgraded to a more advanced lesions.
Figures and Tables






References
1. Liberman L. Clinical management issues in percutaneous core breast biopsy. Radiol Clin North Am. 2000. 38:791–807.

2. MacGrogan G, Moinfar F, Raju V. Tavassoli FA, Devilee P, editors. Intraductal papillary neoplasms. Pathology and Genetics of Tumours of the Breast and Female Genital Organs. 2003. Lyon: IARC;76–80.
3. Rosen EL, Bentley RC, Baker JA, Soo MS. Imaging-guided core needle biopsy of papillary lesions of the breast. AJR Am J Roentgenol. 2002. 179:1185–1192.
4. Ivan D, Selinko V, Sahin AA, Sneige N, Middleton LP. Accuracy of core needle biopsy diagnosis in assessing papillary breast lesions: histologic predictors of malignancy. Mod Pathol. 2004. 17:165–171.
5. Han BK, Choe YH, Ko YH, Yang JH, Nam SJ. Benign papillary lesions of the breast: sonographic-pathologic correlation. J Ultrasound Med. 1999. 18:217–223.
6. Tseng HS, Chen YL, Chen ST, Wu YC, Kuo Sj, Chen LS, et al. The management of papillary lesion of the breast by core needle biopsy. Eur J Surg Oncol. 2009. 35:21–24.
7. Philpotts LE, Shaheen NA, Jain KS, Carter D, Lee CH. Uncommon high-risk lesions of the breast diagnosed at stereotactic core-needle biopsy: clinical importance. Radiology. 2000. 216:831–837.
8. Sydnor MK, Wilson JD, Hijaz TA, Massey HD, Shaw DE, Paredes ES. Underestimation of the presence of breast carcinoma in papillary lesions initially diagnosed at core-needle biopsy. Radiology. 2006. 242:58–62.
9. Ivan D, Selinko V, Sahin AA, Sneige N, Middleton LP. Accuracy of core needle biopsy diagnosis in assessing papillary breast lesions: histologic predictors of malignancy. Mod Pathol. 2004. 17:165–171.
10. Agoff SN, Lawton TJ. Papillary lesions of the breast with and without atypical ductal hyperplasia: can we accurately predict benign behavior from core needle biopsy? Am J Clin Pathol. 2004. 122:440–443.
11. Mercado CL, Hamele-Bena D, Oken SM, Singer CI, Cangiarella J. Papillary lesions of the breast at percutaneous core-needle biopsy. Radiology. 2006. 238:801–808.
12. Bernik SF, Troob S, Ying BL, Simpson SA. Papillary lesions of the breast diagnosed by core needle biopsy: 71 cases with surgical follow-up. Am J Surg. 2009. 197:473–478.
13. Shin HJ, Kim HH, Kim SM, Yang HR, Sohn JH, Kwon GY, et al. Papillary lesions of the breast diagnosed at percutaneous sonographically guided biopsy: comparison of sonographic features and biopsy methods. AJR Am J Roentgenol. 2008. 190:630–636.
14. Parker SH, Jobe WE, Dennis MA, Stavros AT, Johnson KK, Yakes WF. US-guided automatched large-core breast biopsy. Radiology. 1993. 187:507–511.
15. Wu YC, Chen DR, Kuo SJ. Personal experience of ultrasound-guide 14 gauge core biopsy of breast tumor. Eur J Surg Oncol. 2006. 32:715–718.
16. Jacobs TW, Connolly JL, Schnitt SJ. Nonmalignant lesions in breast core needle biopsies: to excise or not to excise? Am J Surg Pathol. 2002. 26:1095–1110.
17. Page DL, Salhany KE, Jensen RA, Dupont WD. Subsequent breast carcinoma risk after biopsy with atypia in a breast papilloma. Cancer. 1996. 78:258–266.
18. Liberman L, Tornos C, Huzjan R, Bartella L, Morris EA, Dershaw DD. Is surgical excision warranted after benign, concordant diagnosis of papilloma at percutaneous breast biopsy? AJR Am J Roentgenol. 2006. 186:1328–1334.
19. Park HL, Kwak JY, Lee SH, Kim JY, Kim KI, Kim WW, et al. Excision of benign breast disease by ultrasound guided vacuum assisted biopsy device (Mammotome). J Korean Surg Soc. 2005. 68:96–101.
20. Park HL, Kwak JY, Jung HK, Lee SH, Shim JY, Kim JY, et al. Is Mammotome excision feasible for benign breast mass bigger than 3 cm in greatest dimension. J Korean Surg Soc. 2006. 70:25–29.
21. Zografos GC, Zagouri F, Sergentanis TN, Nonni A, Michalopoulos NV, Kontogianni P, et al. Diagnosing papillary lesions using vacuum-assisted breast biopsy: Should conservative or surgical management follow? Onkologie. 2008. 31:653–656.
 XML Download
XML Download