

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
During treatment of cancer, some side effects of conventional treatment may limit the ability of the patient to receive the full course of therapy. To reduce the side effects and improve the effectiveness of standard therapy, many complementary or alternative medicines (CAM) have been tried in patient with a variety of cancers.
Mistletoe extracts are among commonly prescribed CAM for cancer patients. Mistletoe is a semiparasitic plant that grows on several types of trees, including apple, oak, maple, elm, pine, and birch. Viscum album L. extract (VAE) was introduced as a possible treatment for cancer in 1920 by Steiner and Wegman.(1) Mistletoe extracts have been shown to kill cancer cells in the laboratory and to boost the immune system.(2-4) In animal studies, activation of natural killer (NK) cells, monocytes/macrophages, T cells and cytokine release have been demonstrated.(5) Although there are numerous reports regarding cytokine secretion induced by VAE in vitro or in animals, there is limited information on the immunostimulatory effects of VAE in vivo, especially used in adjuvant setting after conventional treatment in patients with operable breast cancer. The aim of this study was to assess the immunologic effects of VAE after surgery followed by standard adjuvant chemoradiation therapy in patients with early breast cancer. The immunologic parameters such as interleukin-2 (IL-2), IL-4, IL-6, IL-10, transforming growth factor-beta (TGF-β), and interferon-gamma (IFN-γ) were measured in test group with VAE treatment and in control group.
METHODS
Patients and controls
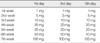
All patients enrolled in this study were diagnosed with stage I or II primary breast cancer and received a standard course of breast conserving surgery, CAF (cyclophosphamide, doxorubicin, and fluorouracil) chemotherapy, and conventional radiation therapy at the department of breast-endocrine surgery of Korea University Medical Center from March 2007 to December 2008. At the time of enrollment, any patient had hematologic abnormality or any other co-morbid condition affecting to immunity was excluded. Total 20 patients were randomly assigned to receive the conventional therapy only (control group, n=10) or the conventional therapy followed by VAE (Helixor®) treatment (test group, n=10). The test group patients started receiving a series of subcutaneous VAE injections two weeks after completion of conventional therapy. VAE was injected three times a week for seven weeks in escalating doses from 1 mg up to 100 mg according to the treatment schedule (Table 1). All patients tolerated the treatment without interruption by the considerable complications such as severe local reaction or fever. Blood samples (5 mL for sera) were collected before and one week after completion of the scheduled VAE injections from test group, and from control group at the corresponding time. The institutional review board of Korea University Anam Hospital approved this study and all patients provided informed consent.
Cytokine measurements
Plasma samples from each patient were collected and stored in a -80℃ freezer until analysis. Measurements of IL-2, IL-4, IL-6, IL-10, TGF-β, and human IFN-γ levels in serum samples from patients were quantified by ELISA (R&D Systems, Abingdon, UK) according to the manufacturer's instructions.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) program (version 14.0; SPSS Inc., Chicago, USA). Descriptive statistics were calculated to summarize the data. The concentrations in each cytokine between before and after VAE treatment in each group were compared with the Wilcoxon signed-rank test. The differences of concentration in each cytokine between test and control group were analyzed by the Mann-Whitney U test. All comparisons were considered significant at p-value <0.05.
RESULTS
Patients' characteristics
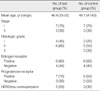
All patients were diagnosed as an invasive ductal carcinoma of breast. One patient of test group had a lobular carcinoma component. The mean age at diagnosis was 46.9 yr, range from 33 to 53 yr in test group and 48.7 yr, range from 41 to 63 yr in control group. Seven patients were stage I and three patients were stage II in each group. Estrogen receptor was positive in six patients in each group (Table 2).
Cytokines results
The mean concentrations of IL-2 were changed from 7.80±1.59 pg/mL and 8.50±2.35 pg/mL before treatment to 8.01±1.45 pg/mL and 7.67±1.76 pg/mL after treatment in the test and control group. But there were not significant differences between both groups and between before and after. The mean concentrations of IL-4 were measured from 11.78±4.04 pg/mL and 13.21±3.48 pg/mL before treatment in the test and control group to 13.81±5.13 pg/mL and 12.92±2.93 pg/mL after treatment. They were statistically not different too. In IL-10, there were also not significant changes, from 20.20±0.61 pg/mL and 20.24±0.76 pg/mL before in the test and control group to 20.43±0.70 pg/mL and 20.07±0.56 pg/mL after. The concentration of TFG-β was increased from 28.25µ15.51 pg/mL to 35.08µ13.54 pg/mL after treatment in test group, but similar change was also measured in control group, from 30.26±12.66 pg/mL to 34.65±10.87 pg/mL. The differences between both groups and between before and after were statistically not significant.
The concentration of IL-6 in the test group was significantly increased from 8.19±1.75 pg/mL to 9.86±1.46 pg/mL after treatment (p=0.013) in contrast to slight decrease from 9.44±2.43 pg/mL to 8.76±1.33 pg/mL in control group (Figure 1). The concentration of IFN-γ was remarkably increased after treatment from 91.76±17.16 pg/mL to 167.42±66.61 pg/mL in the test group (p=0.009), compared to no change from 87.58±11.35 pg/mL to 92.83±15.80 pg/mL in the control group (Figure 2). The change in concentration of IFN-γ after treatment was statistically significant between test group and control group (p=0.002) (Table 3).
DISCUSSION
Impairment in immune function has been demonstrated in cancer patients.(6) In addition, cancer treatment with chemotherapy and radiotherapy generally leads to further immune-suppression. We wondered whether VAE therapy as immunemodulator could lead to improved immunity in immune-compromised patients after chemoradiation. In this study we measured IL-2, IL-6, and IFN-γ as parameters for cell-mediated immunity, IL-4 for humoral immunity, and IL-10 and TGF-β for suppression in immunity.
During the development of the tumor specific immune response, T helper (Th) cells are differentiated in two subsets (Th1 and Th2 cells), depended on cytokines (IL-6, IL-12) secreted by monocytes/dendritic cells. T helper type 1 (Th1) cells are characterized by their hallmark cytokine IFN-γ and are shown to be important for cell-mediated immune responses by their activation of macrophages and the killing of intracellular pathogens. In contrast, Th2 cells produce IL-4 and IL-5, cytokines that they showed are involved in humoral immunity by antibody responses.(7) IL-10 is mainly expressed in monocytes, Th2 cells, and regulatory T cells. It has pleiotropic effects in immunoregulation and inflammation. It down-regulates the expression of Th1 cytokines but enhances B cell survival, proliferation, and antibody production. TGF-β is important in regulation of the immune system by regulatory T cells. It appears to block the activation of monocyte and IL-2 induces the differentiation of cytotoxic T lymphocytes and effects on NK cells. IL-6 also induces the stimulation of cytotoxic T cells and helps in producing lymphokine-activated killer cells. IFN-γ plays a critical role in the immune system. It is produced predominantly by NK cells and natural killer T (NKT) cells as part of the innate immune response.
Several studies have shown the immunological responses to mistletoe extracts in patients with a variety of cancers. Signaling by purified mistletoe lectin induces activation of transcription and secretion of pro-inflammatory cytokines such as IL-1, IL-6, and TNF-α in human peripheral blood mononuclear and endothelial cells.(8) Kovacs(9) showed that treatment with VAE lead an increase in the serum level of IL-12 and an increase of IL-12 and IFN-γ secretion in peripheral blood mononuclear cells. Gardin(10) reported the increases in the number of white blood cells, activated T lymphocytes, complements (C3, C4), immunoglobulins (IgA, IgG, IgM), and delayed hypersensitivity reaction by VAE treatment. The results of this study showed that serum IL-6 and IFN-γ were increased after VAE therapy used in adjuvant setting in patients with breast cancer.
IL-6 is a pleiotropic cytokine that modulates multiple aspects of normal immune and non-immune cell function. Many studies have documented high IL-6 levels in the serum of patients with certain carcinomas (i.e., breast, lung and lymphoma) and have correlated high IL-6 levels with a poor clinical prognosis. In the presence of breast cancer tissue, IL-6 may activate malignant progression of breast cancer cells and enhance metastasis. These data imply an oncogenic role for IL-6. However, the mechanisms involved have not been described.(11-13) By contrast, IL-6 has been reported to induce host immunity involved in the regression of tumors such as melanoma, lung cancer, sarcoma, B lymphoma, and colon cancer.(14-16) The cytolytic activity of NK cells has been reported to be enhanced by IL-6.(17) In immune-compromised animal models, a possible vaccination effect with IL-6 has been reported.(18) VAE stimulates maturation of dendritic cells via secretion of pro-inflammatory cytokines, such as IL-6 and IL-8 in vitro.(19) In this study, because the concentrations of IL-6 in both the test and control groups before VAE treatment were not statistically different and VAE was used after surgical removal of the primary tumor, increased IL-6 concentration appear not to be associated with the tumor, but to be secreted from innate T cells or macrophages under the influence of VAE. This suggests the immunostimulatory effects of VAE.
INF-γ is a cytokine that is involved in promoting both protective immune responses and immune-pathological processes. IFN-γ is produced predominantly by NK cells and NKT cells as part of the innate immune response, and by CD4+ helper and CD8+ cytotoxic T lymphocytes, once antigen specific immunity develops.(20) Lymphocytes and INF-γ have been reported to collaborate in preventing the development of spontaneous intestinal and breast cancers.(21) IFN-γ can exert direct anti-proliferative effects on various tumors. IFN-γ dependent inhibition of cellular proliferation has been observed in human fibrosarcomas and murine fibroblasts.(22) In regard to immunological function, IFN-γ is known as a major macrophage activating factor capable of inducing macrophages to non-specifically kill a variety of tumor cells.(23) In an animal study with mice, production of IFN-γ by activated NKT cells subsequently induced activation of NK cell proliferation and cytolytic activity.(24)
The results of this study showed the increases of IL-6 and IFN-γ levels in peripheral blood by VAE. This suggests that VAE can be used as an immunomodulator in adjuvant setting in patients with breast cancer. However, because this study was carried out on a small numbers of patients, it needs to be confirmed by further studies with a large scale. To more popular use of VAE, further studies for finding out the mechanisms by which VAE increases the immunity will be needed.
CONCLUSION
Significant increases in the serum concentration of IL-6 and IFN-γ were observed after VAE treatment. These results suggest that VAE can stimulate immune responses, especially cell-mediated immunity, in immune-compromised patients received the conventional chemoradiation for breast cancer.



 XML Download
XML Download